Peri-operative management of children and young people taking regular corticosteroid therapy
Flowchart
Introduction
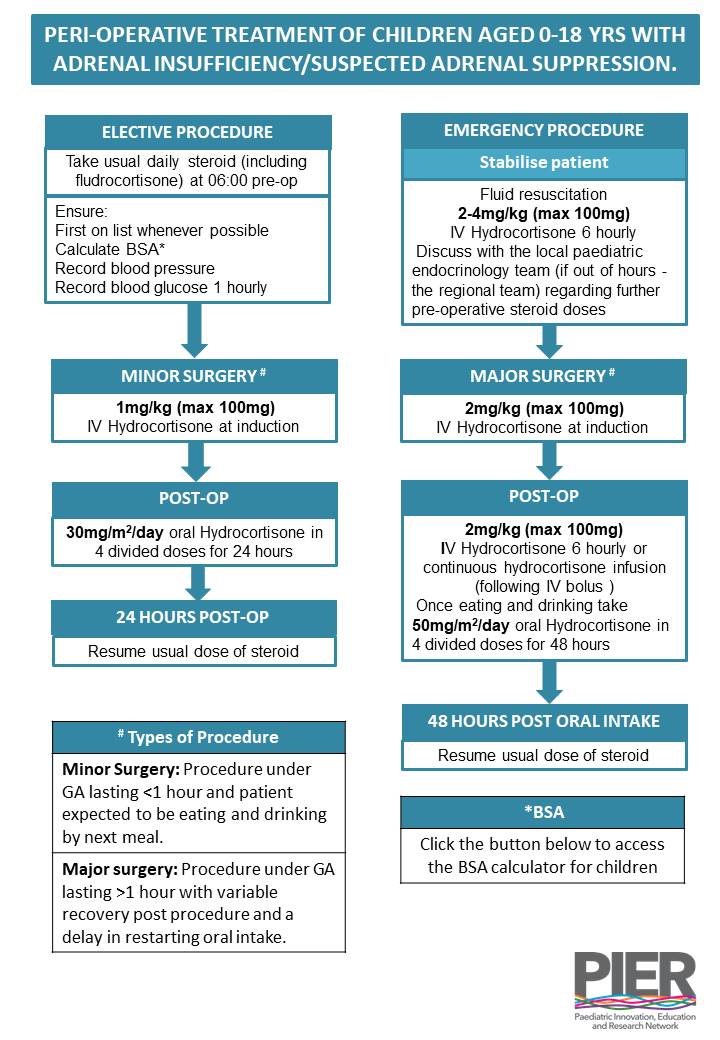
Children and young people (CYP) with adrenal insufficiency or who are at risk of adrenal suppression from long-term corticosteroid therapy may be unable to mount a stress response during surgical procedures that cause major physiological stress, thus additional hydrocortisone cover is required. If managed inappropriately, this can put the CYP at risk of a life-threatening adrenal crisis.
This guideline provides information on the safe use of steroids peri-operatively, and is adapted from BSPED consensus guidance. This guideline covers the following 3 categories:
There are separate PIER guidelines for:
The local paediatrician with a special interest in endocrinology or the regional paediatric endocrinology team at Southampton can be contacted for additional advice. During normal working hours the Southampton Childrens Hospital on call paediatric endocrinology consultant can be contacted via the switchboard. The registrar carries bleep 2027 and the paediatric endocrine nurse specialists (PENS) are on extension 8719. Both are contactable via the hospital switchboard.
This guideline has been developed based on national and international current best practice and expert opinion. It is summarised in the accompanying flow chart on the PIER website
Children and young people (CYP) with adrenal insufficiency or who are at risk of adrenal suppression from long-term corticosteroid therapy may be unable to mount a stress response during surgical procedures that cause major physiological stress, thus additional hydrocortisone cover is required. If managed inappropriately, this can put the CYP at risk of a life-threatening adrenal crisis.
This guideline provides information on the safe use of steroids peri-operatively, and is adapted from BSPED consensus guidance. This guideline covers the following 3 categories:
- Major surgery under general anaesthesia (GA)
- Minor surgery/procedure under GA
- Minor surgery/procedure under local anaesthesia (LA) or non-anaesthetic sedation
There are separate PIER guidelines for:
- Management of Sick Day Episodes in Children and Young People Treated with Regular Glucocorticoids
- Management of adrenal crisis (new presentation or with pre-existing adrenal insufficiency)
The local paediatrician with a special interest in endocrinology or the regional paediatric endocrinology team at Southampton can be contacted for additional advice. During normal working hours the Southampton Childrens Hospital on call paediatric endocrinology consultant can be contacted via the switchboard. The registrar carries bleep 2027 and the paediatric endocrine nurse specialists (PENS) are on extension 8719. Both are contactable via the hospital switchboard.
This guideline has been developed based on national and international current best practice and expert opinion. It is summarised in the accompanying flow chart on the PIER website
Scope
All staff working in Child Health within the Wessex region, anaesthetists, surgeons and theatre staff involved in perioperative care of children up to the age of 18 years
All staff working in Child Health within the Wessex region, anaesthetists, surgeons and theatre staff involved in perioperative care of children up to the age of 18 years
Purpose
The guideline is relevant for children and young people requiring surgery:
The guideline is relevant for children and young people requiring surgery:
- who have known adrenal insufficiency taking daily replacement corticosteroids (usually given as hydrocortisone)
- who will be at risk of adrenal suppression from taking regular corticosteroids (e.g. prednisolone, deflazacort) as treatment for their underlying condition
Definitions
Adrenal Insufficiency (AI): AI is characterised by inadequate production of glucocorticoid +/- mineralocorticoid by the adrenal gland due to a problem at the level of the adrenal gland (primary AI – e.g. congenital adrenal hyperplasia, autoimmune Addison’s disease), pituitary gland (secondary AI – e.g. hypopituitarism) or hypothalamus (tertiary AI). Children with known AI will be on daily doses of hydrocortisone +/- fludrocortisone.
Adrenal Suppression (AS): AS typically occurs due to chronic exogenous steroid use leading to adrenal gland atrophy and inadequate production of endogenous glucocorticoid. AS may be undiagnosed. AS caused by exogenous glucocorticoid use is the most common cause of AI in children. Children at risk of AS will typically be on regular corticosteroids (e.g. prednisolone) for treatment of their underlying illness and will require conversion to oral hydrocortisone around the time of surgery (see Appendix 1)2, which is administered in multiple daily doses to provide a more consistent level of steroid cover.
The main factors that increase the risk of AS in CYP on glucocorticoid therapy can be found in the NPPG (Neonatal & Paediatric Pharmacists Group) position statement on the use of steroid medication warning cards for CYP and can be used to help decide which patients need steroid cover. If you are unsure whether or not a child requires peri-operative steroid cover, please discuss with your local lead for Endocrinology or the regional team in Southampton.
Minor Surgery and Minor Procedures: defined as a procedure lasting less than 90 minutes and the patient is expected to be eating and drinking by the next meal. This may include procedures such as MRI scans, endoscopy, dental extractions under GA or other day case procedures.
Major Surgery: defined as surgery lasting more than 90 minutes with variable recovery periods and expected delay in restarting oral intake.
If you are unsure about the length of anaesthetic or risk of slow post-operative recovery, please discuss with the anaesthetist involved.
Adrenal Insufficiency (AI): AI is characterised by inadequate production of glucocorticoid +/- mineralocorticoid by the adrenal gland due to a problem at the level of the adrenal gland (primary AI – e.g. congenital adrenal hyperplasia, autoimmune Addison’s disease), pituitary gland (secondary AI – e.g. hypopituitarism) or hypothalamus (tertiary AI). Children with known AI will be on daily doses of hydrocortisone +/- fludrocortisone.
Adrenal Suppression (AS): AS typically occurs due to chronic exogenous steroid use leading to adrenal gland atrophy and inadequate production of endogenous glucocorticoid. AS may be undiagnosed. AS caused by exogenous glucocorticoid use is the most common cause of AI in children. Children at risk of AS will typically be on regular corticosteroids (e.g. prednisolone) for treatment of their underlying illness and will require conversion to oral hydrocortisone around the time of surgery (see Appendix 1)2, which is administered in multiple daily doses to provide a more consistent level of steroid cover.
The main factors that increase the risk of AS in CYP on glucocorticoid therapy can be found in the NPPG (Neonatal & Paediatric Pharmacists Group) position statement on the use of steroid medication warning cards for CYP and can be used to help decide which patients need steroid cover. If you are unsure whether or not a child requires peri-operative steroid cover, please discuss with your local lead for Endocrinology or the regional team in Southampton.
Minor Surgery and Minor Procedures: defined as a procedure lasting less than 90 minutes and the patient is expected to be eating and drinking by the next meal. This may include procedures such as MRI scans, endoscopy, dental extractions under GA or other day case procedures.
Major Surgery: defined as surgery lasting more than 90 minutes with variable recovery periods and expected delay in restarting oral intake.
If you are unsure about the length of anaesthetic or risk of slow post-operative recovery, please discuss with the anaesthetist involved.
Background
The Hypothalamic-Pituitary-Adrenal (HPA) Axis
Corticotrophin Releasing Hormone (CRH) secreted by the hypothalamus stimulates the secretion of Adrenocorticotrophic Hormone (ACTH) from the anterior pituitary which in turn causes the release of cortisol from the adrenal cortex. Negative feedback occurs at the level of both the pituitary and hypothalamus in response to raised cortisol levels. Exogenous steroids also cause inhibition of CRH and ACTH release which, if prolonged, causes adrenal atrophy and suppresses the ability of the adrenal glands to increase the production of cortisol in response to stress. Cortisol has many important functions including maintenance of blood pressure and blood glucose levels.
In adults with an intact HPA, the production of cortisol increases from a concentration of 10 mg/day (5.7mg/m2/day) (1,2) to 50 mg/day after minor surgery and 75-150 mg/day after major surgery(3). The cortisol concentration increases during the operation and reaches a peak in the early post-operative period, at the time of anaesthesia reversal and extubation (4,5).
Children with Adrenal Insufficiency
Children with AI, who are known to have a problem with their HPA axis, will be on maintenance doses of hydrocortisone +/- fludrocortisone. Typical maintenance doses of hydrocortisone for CAH are 10-15 mg/m2/day and for other causes of adrenal insufficiency are 8-10 mg/m2/day.
Children with Adrenal Suppression
What is Adrenal Suppression?
Adrenal Suppression (AS) caused by exogenous glucocorticoid use is the most common cause of AI in children. The estimated incidence in the paediatric population is 0.35/100000 (6) but is much higher in the 'at risk' population with 1 in 5 children on long term steroids for Inflammatory Bowel Disease demonstrating biochemical evidence of AS (7). Children on long term glucocorticoid therapy are frequently admitted to hospital for elective surgical procedures such as endoscopy, and require appropriate steroid cover. Children with AS are at risk of an adrenal crisis if they do not receive adequate steroid replacement during stressful events.
Children at risk of AS will typically be on once daily steroids, such as prednisolone, for treatment of their underlying illness and will require conversion to oral hydrocortisone around the time of surgery. This is administered in multiple daily doses and provides a more consistent level of steroid cover.
Who is at risk of Adrenal Suppression?
The following factors have been identified as increasing the risk of AS in children on glucocorticoid therapy and can be used to help decide which patients need steroid cover:
If you are unsure whether or not a child requires perioperative steroid cover based on the above, please discuss with your local paediatrician with a special interest in endocrinology or the regional team in Southampton.
The Hypothalamic-Pituitary-Adrenal (HPA) Axis
Corticotrophin Releasing Hormone (CRH) secreted by the hypothalamus stimulates the secretion of Adrenocorticotrophic Hormone (ACTH) from the anterior pituitary which in turn causes the release of cortisol from the adrenal cortex. Negative feedback occurs at the level of both the pituitary and hypothalamus in response to raised cortisol levels. Exogenous steroids also cause inhibition of CRH and ACTH release which, if prolonged, causes adrenal atrophy and suppresses the ability of the adrenal glands to increase the production of cortisol in response to stress. Cortisol has many important functions including maintenance of blood pressure and blood glucose levels.
In adults with an intact HPA, the production of cortisol increases from a concentration of 10 mg/day (5.7mg/m2/day) (1,2) to 50 mg/day after minor surgery and 75-150 mg/day after major surgery(3). The cortisol concentration increases during the operation and reaches a peak in the early post-operative period, at the time of anaesthesia reversal and extubation (4,5).
Children with Adrenal Insufficiency
Children with AI, who are known to have a problem with their HPA axis, will be on maintenance doses of hydrocortisone +/- fludrocortisone. Typical maintenance doses of hydrocortisone for CAH are 10-15 mg/m2/day and for other causes of adrenal insufficiency are 8-10 mg/m2/day.
Children with Adrenal Suppression
What is Adrenal Suppression?
Adrenal Suppression (AS) caused by exogenous glucocorticoid use is the most common cause of AI in children. The estimated incidence in the paediatric population is 0.35/100000 (6) but is much higher in the 'at risk' population with 1 in 5 children on long term steroids for Inflammatory Bowel Disease demonstrating biochemical evidence of AS (7). Children on long term glucocorticoid therapy are frequently admitted to hospital for elective surgical procedures such as endoscopy, and require appropriate steroid cover. Children with AS are at risk of an adrenal crisis if they do not receive adequate steroid replacement during stressful events.
Children at risk of AS will typically be on once daily steroids, such as prednisolone, for treatment of their underlying illness and will require conversion to oral hydrocortisone around the time of surgery. This is administered in multiple daily doses and provides a more consistent level of steroid cover.
Who is at risk of Adrenal Suppression?
The following factors have been identified as increasing the risk of AS in children on glucocorticoid therapy and can be used to help decide which patients need steroid cover:
- Steroid potency
- Steroid formulations with a more potent glucocorticoid effect and longer half life increase the risk of AS (see appendix 1).
- Route of administration
- Oral steroids increase the risk of AS compared with topical steroids (6).
- High dose inhaled corticosteroids (Beclomethasone and Fluticasone >400mcg daily dose) for more than 3 months have been shown to cause adrenal suppression (8,9).
- Daily dosage
- In adults it is generally accepted that a daily dose of prednisolone >5mg for more than 4 weeks increases the risk for AS (10)
- Supraphysiological doses of glucocorticoid in children would be the equivalent of >10mg/m2/day of hydrocortisone (11).
- Divided and nocturnal doses:
- Multiple daily dosing and administration in the evening increase the risk of AS.
- Duration of treatment
- AS has been documented in children treated for as little as 14 days with oral glucocorticoids12. The risk increases with longer duration of treatment but >4 weeks is significant (13).
- The duration of AS following discontinuation of steroids is variable and can range from between 3 to 18 months (14).
- It is recommended that anyone who has completed a prolonged course of steroids within the last 12 months and has had further short courses of steroids should be considered at risk of AS (15).
- Cushingoid features on examination or features of AI/AS on history (see appendix 2).
If you are unsure whether or not a child requires perioperative steroid cover based on the above, please discuss with your local paediatrician with a special interest in endocrinology or the regional team in Southampton.
Pre-operative Assessment
- When the decision is made to undertake surgery, the surgical team needs to inform the local paediatrician with a special interest in endocrinology (or where appropriate the regional paediatric endocrinology team) and the anaesthetist about the date and time of the planned procedure, the type of procedure and whether it is judged to be major or minor surgery.
- The child should be given first on the list priority to minimise fasting and dehydration which children with AI or AS tolerate poorly.
- No child with AI or AS should be fasted for more than 6 hours.
- If possible, the parents should be contacted prior to surgery to let them know how to manage their child’s steroids at this time (see tables below).
Steroid Dosing Before, During and After Surgery
Pre-operative assessment
When the decision is made to undertake surgery, the surgical team needs to inform the local paediatrician with a special interest in endocrinology or the regional paediatric endocrinology team and the anaesthetist about the date and time of the planned procedure, the type of procedure and whether it is judged to be major or minor surgery (see definitions above).
The child should be given first on the list priority to minimise fasting and dehydration which children with AI or AS tolerate poorly. No child with AI or AS should be fasted for more than 6 hours.
If possible, the parents should be contacted prior to surgery to let them know how to manage their child’s steroids at this time (see tables below).
Pre-operative Fasting
If there is a delay of more than 2 hours in taking the child to theatre, IV maintenance fluids (0.9% sodium chloride plus 5% dextrose) should be started.
General Advice
Children with AI on multiple daily doses of oral hydrocortisone should take their usual dose at 06:00 on the morning of surgery. If the child is taking fludrocortisone this should be given at the same time.
If the child is due any further doses of hydrocortisone routinely while they are in hospital and NBM for the procedure, these should be given intravenously at the usual dose. Please ensure these are prescribed on the drug chart at the time of admission to anticipate any delays.
Children at risk of AS on daily oral prednisolone should be converted to oral hydrocortisone on the day of surgery to provide more consistent cortisol replacement. The first dose should be given at 06:00 prior to theatre.
Minor surgery or minor procedure under GA, morning list
Pre-operative assessment
When the decision is made to undertake surgery, the surgical team needs to inform the local paediatrician with a special interest in endocrinology or the regional paediatric endocrinology team and the anaesthetist about the date and time of the planned procedure, the type of procedure and whether it is judged to be major or minor surgery (see definitions above).
The child should be given first on the list priority to minimise fasting and dehydration which children with AI or AS tolerate poorly. No child with AI or AS should be fasted for more than 6 hours.
If possible, the parents should be contacted prior to surgery to let them know how to manage their child’s steroids at this time (see tables below).
Pre-operative Fasting
- No solid food should be consumed for 6 hours before elective surgery in children.
- In infants, breast milk is safe for up to 4 hours and other milks up to 6 hours. Thereafter, clear fluids should be given as in older children.
- Children should be encouraged to drink clear fluids containing sugar (e.g. sugar containing squash or cranberry juice) up to 1 hour before elective surgery.
- The child’s usual morning dose of hydrocortisone can be given with clear fluids on the morning of surgery and will not interfere with fasting times.
If there is a delay of more than 2 hours in taking the child to theatre, IV maintenance fluids (0.9% sodium chloride plus 5% dextrose) should be started.
General Advice
Children with AI on multiple daily doses of oral hydrocortisone should take their usual dose at 06:00 on the morning of surgery. If the child is taking fludrocortisone this should be given at the same time.
If the child is due any further doses of hydrocortisone routinely while they are in hospital and NBM for the procedure, these should be given intravenously at the usual dose. Please ensure these are prescribed on the drug chart at the time of admission to anticipate any delays.
Children at risk of AS on daily oral prednisolone should be converted to oral hydrocortisone on the day of surgery to provide more consistent cortisol replacement. The first dose should be given at 06:00 prior to theatre.
- For minor surgery a stress dose would be 30 mg/m2/day of hydrocortisone in 4 divided doses (16).
- For major surgery a stress dose would be 50 mg/m2/day of hydrocortisone in 4 divided doses (17).
Minor surgery or minor procedure under GA, morning list
Day Before Surgery |
|
Morning of Surgery |
|
During Surgery |
|
After Surgery |
|
Major Surgery under GA, morning list
Day Before Surgery |
|
Morning of Surgery |
|
During Surgery |
|
After Surgery |
|
Minor Surgery or minor procedure under LA or sedation, morning list e.g. dental extraction
Day Before Surgery |
|
Morning of Surgery |
|
During Surgery |
N/A. Note: MRI scans using non-anaesthetic sedation (e.g. chloral hydrate) does not merit use of IV hydrocortisone – sick day dosing with oral hydrocortisone is sufficient. |
After Surgery |
|
Clinical practice point: fludrocortisone replacement
Some children with adrenal insufficiency take daily fludrocortisone. The above doses of hydrocortisone will provide full mineralocorticoid effect. This means there is no need for additional fludrocortisone cover during surgery. Children should take their usual fludrocortisone on the morning of surgery.
Surgery or Procedures Occurring in the Afternoon
If a procedure is delayed from the morning list and subsequently takes place in the afternoon please remember the following:
- Any further usual doses of hydrocortisone should be given intravenously while the child is NBM in hospital waiting for the procedure.
- Start IV maintenance fluids if the procedure is delayed for more than 2 hours.
- Follow above instructions for major and minor surgery in terms of pre-surgery observations, dosing of hydrocortisone at induction and post-operatively.
If a procedure is scheduled for the afternoon the above advice can still be applied with the following adjustments:
- The child can eat breakfast between 0600-0700 and then follow normal fasting guidelines for milk and clear fluids before the procedure.
- Children should take their usual dose of hydrocortisone (and fludrocortisone) at 0600 on the morning of the procedure.
- Subsequent doses of hydrocortisone, for example the midday dose, should be given intravenously in hospital.
Emergency Surgery
If emergency surgery (e.g. acute appendicitis, treatment of acute fracture) is required, the child should be fluid resuscitated and started on stress doses of IV hydrocortisone at the time of admission (for children >28 days CGA give 1-2mg/kg (max 100mg) 6 hourly; for neonates <28 days CGA give 2-4mg/kg 6 hourly). This dose should be adjusted according to response and/or severity of illness. These children should be resuscitated and stable before going to theatre. Follow the guidance above for major surgery under GA.
Governance
Implementation
The guideline will be displayed on the PIER website and can be accessed by all healthcare professionals working in Wessex. This guideline will be disseminated to consultant paediatric endocrinologists and consultant paediatricians with an interest in endocrinology across Wessex, to share with clinical teams in their hospital.
Process for Monitoring Effectiveness
Compliance with the guideline will be monitored by annual audit at Southampton Childrens Hospital. This will determine whether the guideline is user friendly and identify any changes that need to be made as a result of staff and patient feedback. Audit results will be shared with local and regional endocrinology teams.
The guideline will be reviewed every 3 years or sooner because of audit results or new published evidence.
Implementation
The guideline will be displayed on the PIER website and can be accessed by all healthcare professionals working in Wessex. This guideline will be disseminated to consultant paediatric endocrinologists and consultant paediatricians with an interest in endocrinology across Wessex, to share with clinical teams in their hospital.
Process for Monitoring Effectiveness
Compliance with the guideline will be monitored by annual audit at Southampton Childrens Hospital. This will determine whether the guideline is user friendly and identify any changes that need to be made as a result of staff and patient feedback. Audit results will be shared with local and regional endocrinology teams.
The guideline will be reviewed every 3 years or sooner because of audit results or new published evidence.
References
- Esteban NV, Loughlin T et al. Daily cortisol production rate in man determined by stable isotope dilution/mass spectrometry. J Clin Endocrinol Metab 1991; 72: 39-45.
- Kerrigan JR, Veldhuis JD et al. Estimation of daily cortisol production and clearance rates in normal pubertal males by deconvolution analysis. J Clin Endocrinol Metab 1993; 76: 1505-1510.
- Salem M, Tanish RE et al. Perioperative glucocorticoid coverage. A reassessment 42 years after emergence of a problem. Ann Surg 1994; 219: 416-425.
- Udelsman R, Norton JA et al. Responses of the hypothalamic-pituitary-adrenal and renin-angiotensin axes and the sympathetic system during controlled surgical and anesthetic stress. J Clin Endocrinol Metab 1987: 64; 986-994.
- Jung C, Inder WJ. Management of adrenal insufficiency during the stress of medical illness and surgery. MJA 2008; 188 (7): 409-411.
- Goldbloom E, et al. Symptomatic adrenal suppression among children in Canada. Arch Dis Child. 2017; 102: 340-345.
- Sidoroff M, Kolho K. Screening for adrenal suppression in children with inflammatory bowel disease discontinuing glucocorticoid therapy. BMC Gastroenterology 2014; 14: 51-55.
- Schwartz RH, Neacsu O, Ascher DP, Alpan O. Moderate dose inhaled corticosteroid induced symptomatic adrenal suppression: case report and review of the literature. Clin Pediatr (Phila) 2012; 51: 1184–1190
- Issa-El-Khoury K, Kim H et al. CSACI position statement: systemic effect of inhaled corticosteroids on adrenal suppression in the management of pediatric asthma. Allergy Asthma Clin Immunol 2015; 11: 9.
- Wass JAH, Arlt W. How to avoid precipitating an acute adrenal crisis. BMJ 2012; 345: e6333.
- Goldbloom E, Ahmet A. Adrenal suppression: an under-recognized complication of a common therapy. Paediatr Child Health 2010; 15(7): 411-412.
- Aljebab F et al. Systematic review of the toxicity of short-course oral corticosteroids in children. Arch Dis Child 2016; 101: 365-370.
- Kao J. Adrenal suppression secondary to exogenous glucocorticoids [Internet]. Melbourne, Australia: Royal Children’s Hospital ; August 2015. Available from: www.rch.org.au/uploadedFiles/Main/Content/endo.
- Gordijn MS, Gemke RJ et al. Hypothalamic-pituitary-adrenal (HPA) axis suppression after treatment with glucocorticoid therapy for childhood acute lymphoblastic leukaemia. Cochrane Database Syst Rev 2012; 5: CD008727.
- Hamrahian AH, The management of the surgical patient taking glucocorticoids [Internet]. USA: UpToDate: February 2017. Available from: www.uptodate.com/contents.
- Webb EA, Krone N. Current and novel approaches to children and young people with congenital adrenal hyperplasia and adrenal insufficiency. Best Pract Res Clin Endocrinol Metab. 2015 Jun; 29(3): 449-68
- Park J, Didi M, Blair J. The diagnosis and treatment of adrenal insufficiency during childhood and adolescence. Arch Dis Child 2016; 101: 860-865.
- Great Ormond Street Hospital Clinical Guideline: Perioperative management of children on hydrocortisone replacement.
- Bornstein SR et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2015; 1710: 1-26.
- Chamandari E et al. Congenital adrenal hyperplasia: management during critical illness. Arch Dis Child 2001; 85: 26-28.
Appendix 1:
Equivalent Doses of Commonly Used Glucocorticoids in Relation to Prednisolone
Equivalent Doses of Commonly Used Glucocorticoids in Relation to Prednisolone
This table compares equivalent doses of commonly used glucocorticoids in relation to 5mg of prednisolone, based on their anti-inflammatory properties. It does not take into account mineralocorticoid effects or variations in duration of action of the corticosteroids
Drug |
Dose equivalent to 5mg of prednisolone |
Betamethasone |
750 mcg |
Cortisone acetate |
25 mg |
Deflazacort |
6 mg |
Dexamethasone |
750 mcg |
Hydrocortisone |
20 mg |
Methylprednisolone |
4 mg |
Prednisone |
5 mg |
Triamcinolone |
4 mg |
Appendix 2:
Signs and Symptoms of Adrenal Insufficiency
Cushingoid features for patients on high dose steroids include:
The triad of adrenal crisis is hyponatremia, hyperkalaemia and hypotension.
Clinical features of adrenal insufficiency could include:
Non-specific symptoms
Adapted from Park J et al. Arch Dis Child 2016; 101: 860-86517.
Signs and Symptoms of Adrenal Insufficiency
Cushingoid features for patients on high dose steroids include:
- moon face
- buffalo hump
- abdominal obesity with thin arms and legs
- acne
- fragile skin
- abdominal striae
- hypertension
The triad of adrenal crisis is hyponatremia, hyperkalaemia and hypotension.
Clinical features of adrenal insufficiency could include:
Non-specific symptoms
- Fatigue, vomiting, nausea, abdominal pain, weakness, morning headaches and failure to thrive
- Pallor, sweatiness, disorientation and mood swings
- Dehydration, collapse, hypotension, tachycardia, weight loss, dizziness and salt craving
- Hyperpigmentation of nail beds, mucous membranes, palmer creases and scars
Adapted from Park J et al. Arch Dis Child 2016; 101: 860-86517.
Appendix 3: Calculation of body surface area
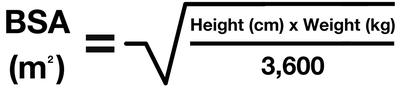
For quick reference use BSA tables in the appendix section of BNFc
Appendix 4:
Hydrocortisone Infusion
Mix 50mls 0.9% Sodium Chloride with 50mg hydrocortisone to give a 1mg/ml solution. A stress dose IV infusion should provide the following doses in 24 hours according to the weight/age of the child:
Hydrocortisone Infusion
Mix 50mls 0.9% Sodium Chloride with 50mg hydrocortisone to give a 1mg/ml solution. A stress dose IV infusion should provide the following doses in 24 hours according to the weight/age of the child:
Weight |
Total dose in 24 hours |
Infusion Rate (mix 50ml 0.9% sodium chloride with 50mg hydrocortisone to give 1mg/ml solution) |
< 10kg |
25mg |
1ml/hr |
10.1-20kg |
50mg |
2ml/hr |
20.1-40kg |
100mg |
4ml/hr |
40.1-70kg |
150mg |
6ml/hr |
Over 70kg |
200mg |
8ml/hr |
Additional Considerations
- Consider more concentrated infusion in those needing fluid restriction (e.g. 100mg hydrocortisone in 50mls 0.9% saline).
- The hydrocortisone infusion can be run alongside 0.9% sodium chloride, 5% glucose and PlasmaLyte solutions.
Adapted from:
- Walker J, Davis E. Emergency Management of Adrenal Failure – Guide for Parents/Community and Ward Professionals. Portsmouth Hospitals NHS Trust.
- Perioperative management of children on hydrocortisone replacement. Great Ormond Street Hospital clinical guideline.
- Webb EA, Krone N. Current and novel approaches to children and young people with congenital adrenal hyperplasia and adrenal insufficiency. Best Pract Res Clin Endocrinol Metab. 2015 Jun; 29(3): 449-68
Appendix 5:
Stat Doses of Intramuscular Hydrocortisone Based on Age
Stat Doses of Intramuscular Hydrocortisone Based on Age
Age |
IM Hydrocortisone Dose (mg) |
<1 year |
25 |
1-5 years |
50 |
>5 years |
100 |
Adapted from the British National Formulary for Children 2018
|
Document Version:
2.0 Lead Author: Dr Anitha Kumaran, Consultant in Paediatric Endocrinology Additional Author: Dr Gemma Watts, Consultant Paediatrician Dr David Lim, SpR Paediatric Endocrinology |
Approving Network:
Wessex Paediatric Endocrine Network Date of Approval: 11/2023 Review Date: 02/2026 |
PIER Contact |
|