Management of children and young people presenting with an adrenal crisis
(new presentation or with pre-existing adrenal insufficiency)
(new presentation or with pre-existing adrenal insufficiency)
Flowchart
Introduction
Presentation with an adrenal crisis is a life-threatening emergency and needs to be managed promptly. An adrenal crisis may present in children and young people (CYP) with pre-existing medical condition that causes adrenal insufficiency or if there is an abrupt cessation of long-term steroid therapy, or it may be the first presentation of undiagnosed adrenal insufficiency.
This guideline is adapted from the BSPED consensus guidance on the management of adrenal crisis1. Young people (16-18 years) admitted under the care of adult services should be managed as per the Society For Endocrinology guidelines
There are separate PIER guidelines for:
Presentation with an adrenal crisis is a life-threatening emergency and needs to be managed promptly. An adrenal crisis may present in children and young people (CYP) with pre-existing medical condition that causes adrenal insufficiency or if there is an abrupt cessation of long-term steroid therapy, or it may be the first presentation of undiagnosed adrenal insufficiency.
This guideline is adapted from the BSPED consensus guidance on the management of adrenal crisis1. Young people (16-18 years) admitted under the care of adult services should be managed as per the Society For Endocrinology guidelines
There are separate PIER guidelines for:
Scope
All staff working in Child Health within the Wessex region involved in the care of CYP up to the age of 18 years. CYP with an adrenal crisis should be discussed with the lead for paediatric endocrinology at each DGH during working hours. See Wessex Paediatric Endocrine Network webpage.
All staff working in Child Health within the Wessex region involved in the care of CYP up to the age of 18 years. CYP with an adrenal crisis should be discussed with the lead for paediatric endocrinology at each DGH during working hours. See Wessex Paediatric Endocrine Network webpage.
Purpose
To improve early diagnosis, clinical outcomes and provide an agreed clinical approach to managing CYP presenting with acute adrenal insufficiency or an adrenal crisis.
To improve early diagnosis, clinical outcomes and provide an agreed clinical approach to managing CYP presenting with acute adrenal insufficiency or an adrenal crisis.
Definitions
Adrenal insufficiency: Inadequate production of glucocorticoid and/or mineralocorticoid by the adrenal gland due to a problem at the level of the adrenal gland (primary), pituitary gland (secondary) or hypothalamus (tertiary).
Adrenal crisis: Adrenal (“Addisonian”) crisis occurs when the adrenal glands cannot produce sufficient cortisol in response to an increased need. The major clinical features of adrenal crisis are hypotension and volume depletion. Combined glucocorticoid and mineralocorticoid deficiency results in urinary sodium loss, hyponatremia, hyperkalaemia, increased serum urea, and, especially in children, hypoglycaemia. Not all features may be present.
Adrenal insufficiency: Inadequate production of glucocorticoid and/or mineralocorticoid by the adrenal gland due to a problem at the level of the adrenal gland (primary), pituitary gland (secondary) or hypothalamus (tertiary).
Adrenal crisis: Adrenal (“Addisonian”) crisis occurs when the adrenal glands cannot produce sufficient cortisol in response to an increased need. The major clinical features of adrenal crisis are hypotension and volume depletion. Combined glucocorticoid and mineralocorticoid deficiency results in urinary sodium loss, hyponatremia, hyperkalaemia, increased serum urea, and, especially in children, hypoglycaemia. Not all features may be present.
Background
Control of cortisol secretion
Corticotrophin releasing hormone (CRH) secreted by the hypothalamus stimulates adrenocorticotrophic hormone (ACTH) secretion from the anterior pituitary, which then stimulates cortisol production from the adrenal cortex. Negative feedback occurs at the pituitary and hypothalamus in response to raised cortisol levels. Cortisol has many important functions including maintenance of blood pressure, blood glucose levels and immunity.
Exogenous steroids will may cause inhibition of CRH and ACTH release, which if prolonged may lead to adrenal atrophy and suppresses the ability of the adrenal glands to increase the production of cortisol in response to stress, leading to primary and secondary adrenal insufficiency.
Classification of adrenal insufficiency
As the future management will differ depending on the underlying cause, it is a key management step to identify whether the initial presentation is either primary adrenal insufficiency (associated with an elevated ACTH) or secondary adrenal insufficiency (associated with an inappropriately normal or low ACTH). It is therefore important to take an ACTH sample at presentation (EDTA sample) and other samples (see below) prior to treatment with hydrocortisone.
Primary adrenal insufficiency (AI): These are disorders of the adrenal gland e.g. autoimmune adrenal insufficiency (Addison's disease), congenital adrenal hyperplasia, steroid-induced adrenal suppression. It typically leads to an elevated ACTH at presentation which may (but not always) manifest as hyperpigmentation.
Secondary adrenal insufficiency: this occurs due to pathologies of the pituitary gland where a lack of ACTH leads to cortisol deficiency, e.g. congenital hypopituitarism, brain tumour, acquired (traumatic brain injury, meningitis). At presentation there is an inappropriately normal or low ACTH.
Tertiary adrenal insufficiency: this may result from long-term exogenous high-dose glucocorticoid use, leading to ACTH suppression. Glucocorticoids are utilised for various indications in children, and administration by any route can cause AI. Defining the paediatric patients on long-term glucocorticoid therapy at risk of adrenal crisis is outside the scope of this guidance; there is published guidance for children and for those prescribed inhaled corticosteroids.
Adrenal Crisis: this occurs when the adrenal glands cannot produce sufficient cortisol in response to an increased need. It is life-threatening and may lead to death. In paediatric patients, an adrenal crisis is defined as:
Clinicians should also be mindful of symptomatic adrenal insufficiency, which may be a precursor to adrenal crisis. Here the child is unwell but not yet having an adrenal crisis, and is often admitted to hospital for treatment of milder symptoms, such as postural dizziness, nausea and abdominal discomfort, lassitude, or poor feeding (in younger patients).
Control of cortisol secretion
Corticotrophin releasing hormone (CRH) secreted by the hypothalamus stimulates adrenocorticotrophic hormone (ACTH) secretion from the anterior pituitary, which then stimulates cortisol production from the adrenal cortex. Negative feedback occurs at the pituitary and hypothalamus in response to raised cortisol levels. Cortisol has many important functions including maintenance of blood pressure, blood glucose levels and immunity.
Exogenous steroids will may cause inhibition of CRH and ACTH release, which if prolonged may lead to adrenal atrophy and suppresses the ability of the adrenal glands to increase the production of cortisol in response to stress, leading to primary and secondary adrenal insufficiency.
Classification of adrenal insufficiency
As the future management will differ depending on the underlying cause, it is a key management step to identify whether the initial presentation is either primary adrenal insufficiency (associated with an elevated ACTH) or secondary adrenal insufficiency (associated with an inappropriately normal or low ACTH). It is therefore important to take an ACTH sample at presentation (EDTA sample) and other samples (see below) prior to treatment with hydrocortisone.
Primary adrenal insufficiency (AI): These are disorders of the adrenal gland e.g. autoimmune adrenal insufficiency (Addison's disease), congenital adrenal hyperplasia, steroid-induced adrenal suppression. It typically leads to an elevated ACTH at presentation which may (but not always) manifest as hyperpigmentation.
Secondary adrenal insufficiency: this occurs due to pathologies of the pituitary gland where a lack of ACTH leads to cortisol deficiency, e.g. congenital hypopituitarism, brain tumour, acquired (traumatic brain injury, meningitis). At presentation there is an inappropriately normal or low ACTH.
Tertiary adrenal insufficiency: this may result from long-term exogenous high-dose glucocorticoid use, leading to ACTH suppression. Glucocorticoids are utilised for various indications in children, and administration by any route can cause AI. Defining the paediatric patients on long-term glucocorticoid therapy at risk of adrenal crisis is outside the scope of this guidance; there is published guidance for children and for those prescribed inhaled corticosteroids.
Adrenal Crisis: this occurs when the adrenal glands cannot produce sufficient cortisol in response to an increased need. It is life-threatening and may lead to death. In paediatric patients, an adrenal crisis is defined as:
- an acute deterioration in health; and
- associated with either acute haemodynamic disturbance (hypotension or sinus tachycardia relative to age-related normal levels), marked abnormality in one or more electrolytes (hyponatraemia, hyperkalaemia), or hypoglycaemia; and
- that is not attributable to another illness; and
- the features of which show significant resolution following parenteral glucocorticoid administration.
Clinicians should also be mindful of symptomatic adrenal insufficiency, which may be a precursor to adrenal crisis. Here the child is unwell but not yet having an adrenal crisis, and is often admitted to hospital for treatment of milder symptoms, such as postural dizziness, nausea and abdominal discomfort, lassitude, or poor feeding (in younger patients).
Key Points for the assessment of a child with suspected adrenal crisis
Clinical Features of adrenal insufficiency or an adrenal crisis
These may be evident as deficiency of cortisol, aldosterone or both.
- The diagnosis of adrenal crisis should be considered in a child presenting with shock, hypotension and volume depletion, hyponatraemia, hyperkalaemia (not always present), hypoglycaemia and increased serum urea and creatinine.
- Symptoms may initially be also non-specific and include a more insidious onset with recurrent infections, recurrent episodes of hypoglycaemia or hyponatraemia, growth faltering, lethargy, poor feeding, weight loss, abdominal pain and vomiting. Features of aldosterone deficiency include salt craving, muscle weakness and dizziness.
- An adrenal crisis is often triggered by intercurrent illness such as gastroenteritis or infection, trauma, or non-compliance with steroid replacement therapy.
- Some conditions can mimic the presentation of adrenal insufficiency such as sepsis, obstructive uropathy (in neonates) and pseudohypoaldosteronism – therefore it is important that correct samples are taken prior to treatment with hydrocortisone to determine aetiology of the presentation.
- The future management of a child with adrenal insufficiency/adrenal crisis will differ depending on the underlying aetiology (i.e. primary versus secondary adrenal insufficiency) – this emphasises again importance of taking the correct samples prior to treatment with hydrocortisone.
Clinical Features of adrenal insufficiency or an adrenal crisis
These may be evident as deficiency of cortisol, aldosterone or both.
|
Infants:
Hypoglycaemia Jaundice Neonatal hepatitis Poor feeding Weight faltering Hyperpigmentation Collapse, death |
Child:
Nausea, vomiting Weight loss, anorexia Hypotension, Postural hypotension Hypoglycaemia Worsening fatigue Hyperpigmentation Collapse, death History of recurrent infections |
Features of aldosterone deficiency:
Muscle weakness, fatigue, weight loss, nausea and vomiting, salt craving, hypotension/dizziness, hyponatraemia, hyperkalaemia, acidosis.
Muscle weakness, fatigue, weight loss, nausea and vomiting, salt craving, hypotension/dizziness, hyponatraemia, hyperkalaemia, acidosis.
Guideline for the Management of an adrenal crisis
Implementation
- `This guideline will be disseminated through the Wessex Paediatric Endocrine Network. The network centre lead at each DGH will inform their department the guideline is available.
Process for Monitoring Effectiveness
- Effectiveness of the guideline will be monitored by feedback to the lead author.
Appendix 1: IV Hydrocortisone Infusion
Weight |
Total Dose in 24 Hours |
Infusion Rate (mix 50ml 0.9% sodium chloride with 50mg hydrocortisone to give 1mg/ml solution) |
≤10kg |
25mg |
1ml/hr |
10.1-20kg |
50mg |
2 ml/hr |
20.1-40kg |
100mg |
4ml/hr |
40.1-70kg |
150mg |
6ml/hr |
Over 70kg |
200mg |
8ml/hr |
Additional considerations
- Consider more concentrated infusion in those needing fluid restriction (e.g. 100mg hydrocortisone in 50mls 0.9% saline).
- The hydrocortisone infusion can be run alongside 0.9% sodium chloride, 5% glucose and PlasmaLyte solutions
Appendix 2: Management of fluid and electrolyte abnormalities in primary and secondary AI
Primary Adrenal Insufficiency |
Secondary Adrenal Insufficiency |
|
ACTH Levels |
Elevated |
Suppressed |
Glucocorticoid treatment |
Usually hydrocortisone |
Usually hydrocortisone (or prednisolone) |
Mineralocorticoid treatment |
Fludrocortisone |
Not required |
During Acute Illness:
Primary Adrenal Insufficiency |
Secondary Adrenal Insufficiency |
|
Possible sodium and potassium abnormalities |
|
|
Other possible electrolyte abnormalities |
|
|
Treatment |
|
|
Features warranting slow or particularly careful rehydration in hyponatraemia:
Key Considerations in severe hyponatraemia:
- Rapid correction of acute and chronic hyponatraemia can be associated with a significant risk of cerebral oedema and/or osmotic demyelination syndrome
- There is a substantial risk of seizures with plasma Na <110 mmol/l and an elevated risk of the osmotic demyelination syndrome if plasma Na concentration <105 mmol/l
- A careful approach to rehydration is therefore needed in children with: a) Severe hyponatraemia; plasma sodium < 120 mmol/l; b) Reduced consciousness, seizures or other signs compatible with cerebral oedema; c) Diabetes insipidus; d) When duration of illness or being unwell is more than one day.
Key Considerations in severe hyponatraemia:
- Avoid increasing plasma Na concentration by >10 mmol/l/day (~0.5 mmol/l/hr) in these circumstances. Normal (0.9%) saline with stress doses of glucocorticoid can increase sodium concentrations more rapidly than this. Therefore, the IV fluid may need to be changed to one containing less sodium
- A slow, measured, increase in serum sodium can be achieved by linking sodium input (fluid) to output (urine) (i.e. giving a little more sodium than that present in the urine)
- In patients in adrenal crisis careful monitoring of electrolytes is required. This is particularly important when hydrocortisone treatment is started because in addition to its mineralocorticoid action, hydrocortisone will also switch off ADH secretion leading to a diuresis and potentially a rapid rise in plasma sodium concentration
- 1ml/kg of 3% saline will increase the plasma Na concentration by about 1 mmol/l. This can be considered especially in the context of abnormal neurology or ongoing severe symptomatic hyponatraemia. This bolus may need to be repeated. Close supervision and regular clinical assessment and monitoring of electrolytes is required
- Consider admission to PHDU/PICU
- The rate of correction of hyponatraemia may be dependent on the underlying aetiology. The sodium should not rise >10mmol/l in 24 hours
Appendix 3: Calculation of body surface area (BSA)
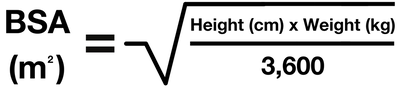
- For quick reference use BSA tables in the appendix section on BNFc.
Appendix 4: Checklist prior to hospital discharge
References
- BSPED. Available from: https://www.bsped.org.uk/media/yqnpvaix/bsped-paediatric-adrenal-insufficiency-guidance-2023.pdf
- BNFc. Available from: https://bnfc.nice.org.uk/drugs/hydrocortisone/
- Neonatal and paediatric pharmacy group (NPPG). Available from: http://nppg.org.uk/wp- content/uploads/2021/12/Position-Statement-Steroid-Cards-V1.pdf
- SIGN. Available from: www.sign.ac.uk/media/1773/sign158-updated.pdf
- National Institute of Clinical Excellence (NICE). Available from: www.nice.org.uk/guidance/ ng80/evidence/chronic-asthma-management-pdf-7079863934
- Rushworth RL, Torpy DJ, Stratakis CA, et al. Adrenal crises in children: perspectives and research directions. Horm Res Paediatr 2018;89:341–51.
- Emergency and perioperative management of adrenal insufficiency in children and young people: British Society for Paediatric Endocrinology and Diabetes consensus guidance
- T Mushtaq, SR Ali, N Boulos, R Boyle, T Cheetham, JH Davies, CJ Elder, H-W Gan, PC Hindmarsh, H Katugampola, N Krone, M Salomon Estebanez, S Shenoy, S Tollerfield, SC Wong, F Regan; Developed by the Paediatric Adrenal Insufficiency Group on behalf of the British Society for Paediatric Endocrinology and Diabetes (BSPED) 2023
Arch Dis Child Nov;108(11):871-878. doi: 10.1136/archdischild-2022-325156. Epub 2023 Apr 12.
|
Document Version:
2.0 Lead Author: Dr Ed Hind, Consultant Paediatrician Co-Author: Dr David Lim, SpR Paediatric Endocrinology Professor Justin Davies, Consultant Paediatric Endocrinologist |
Approving Network:
Wessex Paediatric Endocrine Network Date of Approval: 11/2023 Review Date: 11/2026 |
PIER Contact |
|