Management of Sick Day Episodes in Children and Young People Treated with Regular Glucocorticoids
Introduction
This guideline is intended for doctors providing advice for children and young people (CYP) with known or risk of adrenal insufficiency who are on long-term glucocorticoid therapy for a long-term condition, during intercurrent illness or trauma (i.e. sick day episodes).
In these situations, these CYP may be unable to mount an endogenous cortisol response to stress. Thus extra steroid is required in the form of hydrocortisone, given either orally, intramuscularly or intravenously depending on the severity of the clinical situation. If not managed appropriately, it is potentially life-threatening.
This guideline is adapted from the BSPED consensus guidance on the management of adrenal insufficiency which includes steroid management of sick day episodes1. Separate PIER guidelines exist for the management on adrenal crisis and peri-operative steroid management for this group of CYP.
This guideline is intended for doctors providing advice for children and young people (CYP) with known or risk of adrenal insufficiency who are on long-term glucocorticoid therapy for a long-term condition, during intercurrent illness or trauma (i.e. sick day episodes).
In these situations, these CYP may be unable to mount an endogenous cortisol response to stress. Thus extra steroid is required in the form of hydrocortisone, given either orally, intramuscularly or intravenously depending on the severity of the clinical situation. If not managed appropriately, it is potentially life-threatening.
This guideline is adapted from the BSPED consensus guidance on the management of adrenal insufficiency which includes steroid management of sick day episodes1. Separate PIER guidelines exist for the management on adrenal crisis and peri-operative steroid management for this group of CYP.
Scope
Paediatricians working in paediatric endocrinology network centres across Wessex.
Paediatricians working in paediatric endocrinology network centres across Wessex.
Purpose
The aim of the guideline is to provide an agreed clinical approach to managing children at home who take regular oral corticosteroids and who have an intercurrent illness or trauma, to enable prompt assessment in hospital where required, improve patient experience and clinical outcomes.
The aim of the guideline is to provide an agreed clinical approach to managing children at home who take regular oral corticosteroids and who have an intercurrent illness or trauma, to enable prompt assessment in hospital where required, improve patient experience and clinical outcomes.
Key Practice Points
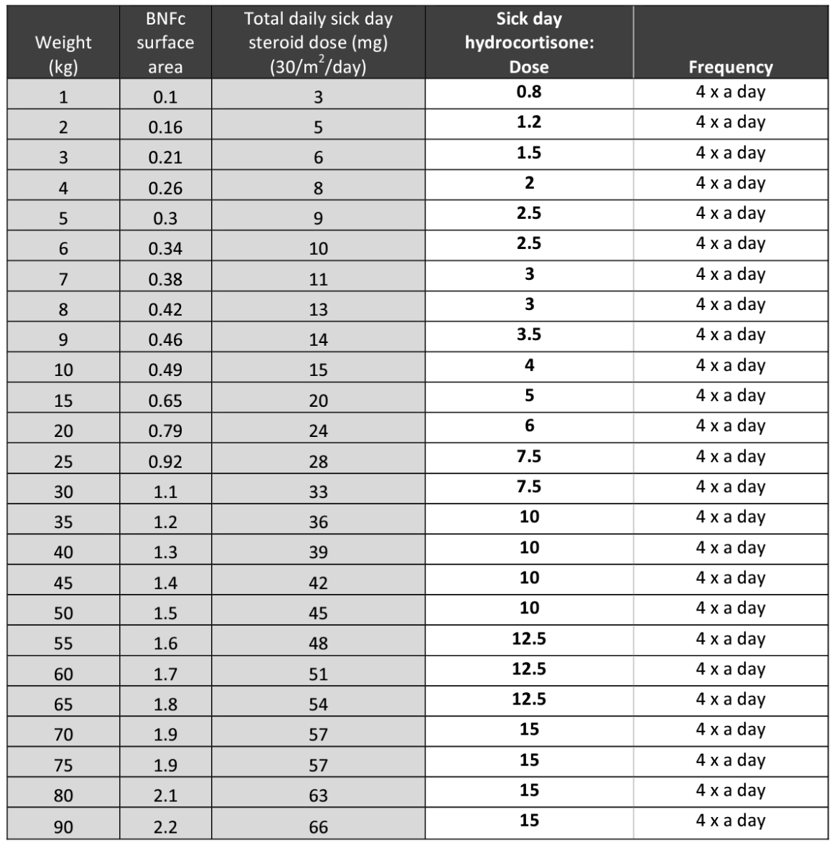
- The recommended management of sick day episodes is a dose-based strategy aiming for a total daily hydrocortisone dose of around 30mg/m2/day given as four equally divided doses at regular 6 hourly intervals. This avoids long gaps between doses and overcomes the relatively short half-life of oral hydrocortisone, ensuring that adequate plasma levels are maintained during times of stress. See Appendix 1 for calculation of body surface area.
- For patients on enzyme-inducing medications higher sick day doses may be required.
- For those patients taking regular glucocorticoids other than hydrocortisone e.g. prednisolone, deflazacort etc, sick day episode doses of hydrocortisone should be given in addition to their regular glucocorticoid treatment.
- A guide to pre-calculated sick day doses in four equally divided doses is provided in Appendix 2.
- If the child is on twice daily Efmody (modified release hydrocortisone), they should be switched whilst unwell to oral hydrocortisone (standard immediate release preparation) in four divided doses using a dose of 30mg/m2/day.
- If the child is on fludrocortisone (used in primary adrenal insufficiency), the dose does not need adjustment in the event of a sick day episode or an adrenal crisis. Fludrocortisone should be continued as usual. If the child is unable to take oral medication then intravenous fluids may be required to maintain the salt and water balance depending on the clinical situation. However, the mineralocorticoid effect of hydrocortisone at stress doses is often sufficient to cover the mineralocorticoid requirement. Oral fludrocortisone should be re-commenced when tolerated.
- Intramuscular (preparations of hydrocortisone include hydrocortisone sodium succinate (supplied as a powder to be dissolved in water for injection) and hydrocortisone sodium phosphate (available as a liquid preparation).
Table 1: Common situations when additional sick day episode oral and emergency hydrocortisone is recommende
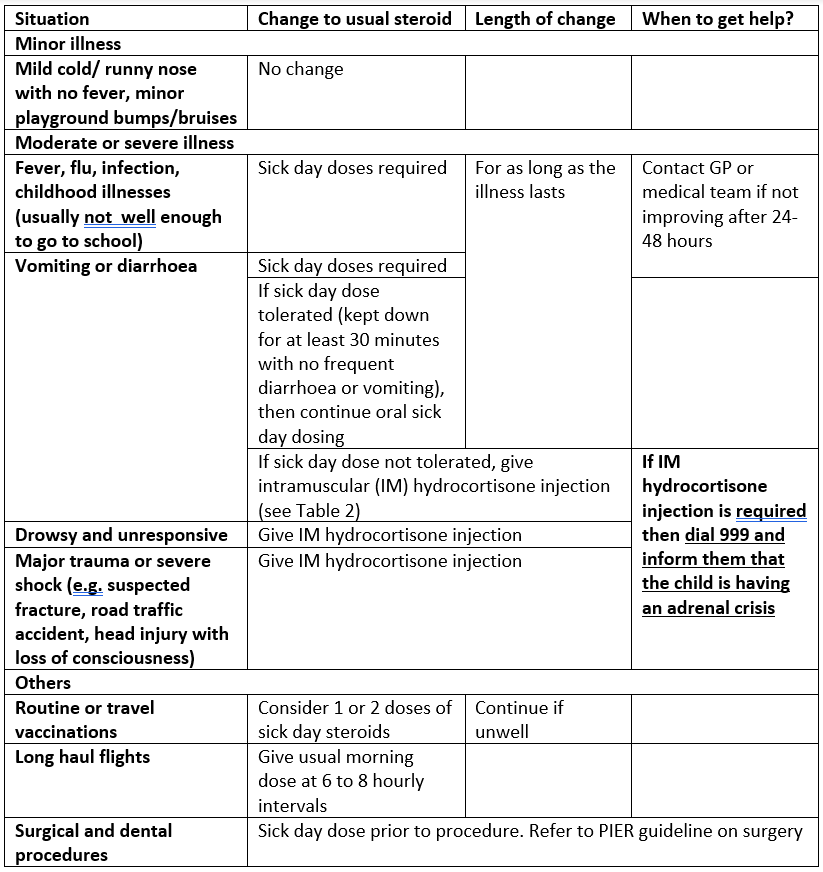
Table 2: Intramuscular (or initial intravenous) hydrocortisone doses given in the community

Implementation
This guideline will be disseminated through the Wessex Paediatric Endocrine Network. The network centre lead at each DGH will inform their department the guideline is available.
This guideline will be disseminated through the Wessex Paediatric Endocrine Network. The network centre lead at each DGH will inform their department the guideline is available.
Process for Monitoring Effectiveness
Effectiveness of the guideline will be monitored by feedback to the lead author.
Effectiveness of the guideline will be monitored by feedback to the lead author.
Appendix 1: Calculation of Body Surface Area
- BSA (m2) = Square root of (weight in kg x height in cm/3600)
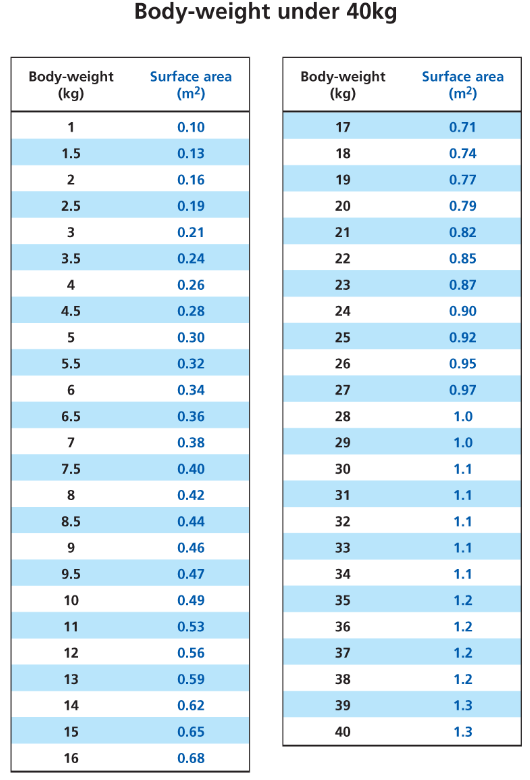
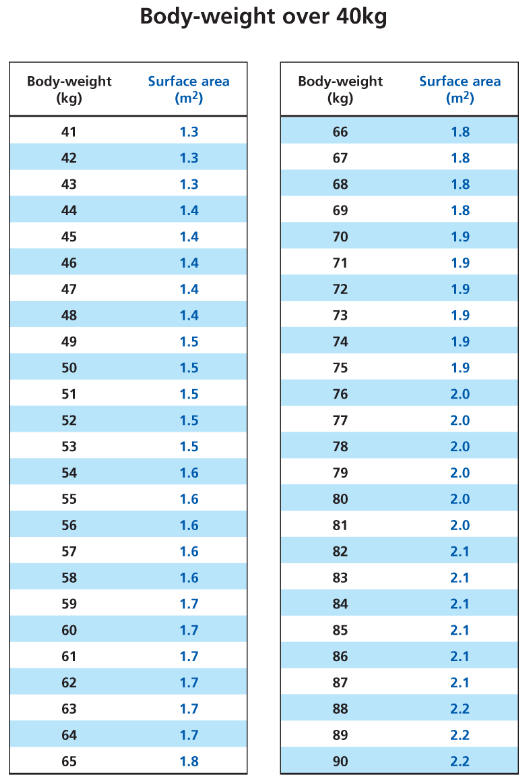
- For quick reference use BSA tables in the appendix section on BNFc (below)
|
|
Appendix 2: Pre-calculated Hydrocortisone sick day doses for a range of weights
References
- BSPED. Available from: https://www.bsped.org.uk/media/yqnpvaix/bsped-paediatric-adrenal-insufficiency-guidance-2023.pdf
- NICE. Available from: https://cks.nice.org.uk/topics/corticosteroids-oral/background-information/equivalent-anti-inflammatory-doses/
- Emergency and perioperative management of adrenal insufficiency in children and young people: British Society for Paediatric Endocrinology and Diabetes consensus guidance
- Talat Mushtaq , Salma R Ali, Nabil Boulos , Roisin Boyle, Tim Cheetham, Justin Huw Davies, Charlotte Jane Elder, Hoong-Wei Gan, Peter C Hindmarsh, Harshini Katugampola, Nils Krone, Maria Salomon Estebanez, Savitha Shenoy, Sally Tollerfield, Sze Choong Wong, Fiona Regan; Developed by the Paediatric Adrenal Insufficiency Group on behalf of the British Society for Paediatric Endocrinology and Diabetes (BSPED)
Arch Dis Child. 2023 Apr 12:archdischild-2022-325156. doi: 10.1136/archdischild-2022-325156. Online ahead of print.
|
Document Version:
2.0 Lead Author: Dr Justin Davies, Consultant Paediatric Endocrinologist Additional Author: Dr David Lim, Paediatric Endocrinology GRID trainee |
PIER Contact |
|