Investigations and Initial Management of Hypoglycaemia
Introduction
This guideline is intended to provide doctors with a clear structure for the initial investigations and management of babies, infants and children who present with hypoglycaemia. It incorporates recently published guidance and consensus.
This guideline excludes those with insulin dependent diabetes or a known metabolic disorder and babies with early onset hypoglycaemia <72 hours of birth for which there is separate neonatal guidance.
There is a separate PIER guideline for neonatal hyperinsulinaemic hypoglycaemia here - https://www.piernetwork.org/hyperinsulinaemic-hypoglycaemia-in-neonates.html
This guideline is intended to provide doctors with a clear structure for the initial investigations and management of babies, infants and children who present with hypoglycaemia. It incorporates recently published guidance and consensus.
This guideline excludes those with insulin dependent diabetes or a known metabolic disorder and babies with early onset hypoglycaemia <72 hours of birth for which there is separate neonatal guidance.
There is a separate PIER guideline for neonatal hyperinsulinaemic hypoglycaemia here - https://www.piernetwork.org/hyperinsulinaemic-hypoglycaemia-in-neonates.html
Scope
Paediatricians working across Wessex. Children with hypoglycaemia should be discussed with the DGH lead for paediatric endocrinology at each DGH during working hours
Paediatricians working across Wessex. Children with hypoglycaemia should be discussed with the DGH lead for paediatric endocrinology at each DGH during working hours
Purpose
To provide an agreed clinical approach to managing hypoglycaemia, provide a structured overview of underlying disorders that can result in hypoglycaemia and guide clinicians to the appropriate investigations including those that are time critical and must be carried out at the time of hypoglycaemia and prior to initiating treatment.
To provide an agreed clinical approach to managing hypoglycaemia, provide a structured overview of underlying disorders that can result in hypoglycaemia and guide clinicians to the appropriate investigations including those that are time critical and must be carried out at the time of hypoglycaemia and prior to initiating treatment.
Definitions
Normoglycaemia
Other than the first 2-3 days of life normal fasting blood glucose is kept within a narrow physiological range 3.5-5.5 mmol/l.
Hypoglycaemia
Clinical hypoglycaemia is defined as blood glucose (BG) concentration low enough to cause symptoms and or signs of impaired brain function. It cannot be defined by a specific BG level as thresholds for specific brain responses to hypoglycaemia occur across a range of BG levels and can be influenced by the presence of alternative fuels such as ketones or lactate.
Neurogenic symptoms are perceived at a BG concentration < 3.0mmol/l, which in older children and adults triggers a search for food or assistance.
Cognitive function is impaired at a BG concentration < 2.8mmol/l.
Young infants and children often cannot dependably recognize and or communicate their symptoms.
A BG < 2.6 mmol/l is generally regarded as a level at which prompt investigation and treatment is required regardless of the presence of symptoms.
Glucose homeostasis
The key hormones that regulate glucose homeostasis are insulin, glucagon, adrenaline, noradrenaline, cortisol and growth hormone. Insulin regulates glucose homeostasis in the post prandial state whereas the other hormones (counter regulatory hormones) control glucose levels during the fasting state. Glucagon and adrenaline are the main line of defence against hypoglycaemia whereas cortisol and GH have a permissive role in regulating blood glucose levels.
Hypoglycaemia associated autonomic failure (HAAF)
Reduced or absent awareness of hypoglycaemia and impaired hepatic glucose release due to impaired neurogenic responses to hypoglycaemia. This can persist for > 24 hours after a single episode of hypoglycaemia and longer after repeated episodes.
Transitional hypoglycaemia
After birth the continuous glucose delivery to the foetus is disrupted and for the first few hours, after birth there is a transitional phase of physiologically low normal blood glucose levels (transitional hypoglycaemia) which normalises around 72 hours after birth.
Ketone bodies
Acetoacetate and Beta – hydroxybutyrate are produced by beta oxidation of free fatty acids and can be utilised as an alternative energy source. Free fatty acids are released during lipolysis in the fasting state when insulin levels are low. The presence or absence of ketones during hypoglycaemia is key to considering the diagnosis and appropriate further investigations.
Normoglycaemia
Other than the first 2-3 days of life normal fasting blood glucose is kept within a narrow physiological range 3.5-5.5 mmol/l.
Hypoglycaemia
Clinical hypoglycaemia is defined as blood glucose (BG) concentration low enough to cause symptoms and or signs of impaired brain function. It cannot be defined by a specific BG level as thresholds for specific brain responses to hypoglycaemia occur across a range of BG levels and can be influenced by the presence of alternative fuels such as ketones or lactate.
Neurogenic symptoms are perceived at a BG concentration < 3.0mmol/l, which in older children and adults triggers a search for food or assistance.
Cognitive function is impaired at a BG concentration < 2.8mmol/l.
Young infants and children often cannot dependably recognize and or communicate their symptoms.
A BG < 2.6 mmol/l is generally regarded as a level at which prompt investigation and treatment is required regardless of the presence of symptoms.
Glucose homeostasis
The key hormones that regulate glucose homeostasis are insulin, glucagon, adrenaline, noradrenaline, cortisol and growth hormone. Insulin regulates glucose homeostasis in the post prandial state whereas the other hormones (counter regulatory hormones) control glucose levels during the fasting state. Glucagon and adrenaline are the main line of defence against hypoglycaemia whereas cortisol and GH have a permissive role in regulating blood glucose levels.
Hypoglycaemia associated autonomic failure (HAAF)
Reduced or absent awareness of hypoglycaemia and impaired hepatic glucose release due to impaired neurogenic responses to hypoglycaemia. This can persist for > 24 hours after a single episode of hypoglycaemia and longer after repeated episodes.
Transitional hypoglycaemia
After birth the continuous glucose delivery to the foetus is disrupted and for the first few hours, after birth there is a transitional phase of physiologically low normal blood glucose levels (transitional hypoglycaemia) which normalises around 72 hours after birth.
Ketone bodies
Acetoacetate and Beta – hydroxybutyrate are produced by beta oxidation of free fatty acids and can be utilised as an alternative energy source. Free fatty acids are released during lipolysis in the fasting state when insulin levels are low. The presence or absence of ketones during hypoglycaemia is key to considering the diagnosis and appropriate further investigations.
Clinical Features of Acute Hypoglycaemia
Hypoglycaemia may be associated with symptoms and signs or may be asymptomatic.
Clinical features associated with symptomatic hypoglycaemia are as follows:
Hypoglycaemia may be associated with symptoms and signs or may be asymptomatic.
Clinical features associated with symptomatic hypoglycaemia are as follows:
Neonates |
Infant/Older Child |
Pallor Sweating Tachypnoea Jitteriness Apnoea Hypotonia Feeding difficulties Irritability Abnormal cry Convusions Coma |
Anxiety Tremor Weakness and lassitude Nausea Vomiting Hunger and abdominal pain Headache Confusion Ataxia Poor concentration Convulsions |
Important Points to Guide the History
The history must be thorough and should include:
The history must be thorough and should include:
- Timing of the episode of hypoglycaemia and its relationship to food (i.e. how long was the fasting episode)
- Features and timing or previous episodes of suspected hypoglycaemia
- Ability to cope with intercurrent illness
- Birth history and weight
- Neonatal jaundice and or hypoglycaemia
- Tolerance to fasting/illness
- Drug ingestion
- Family history parental consanguinity
- History of neonatal or unexplained deaths in the family
Important Clues in the Clinical Examination
- Features of sepsis, hepatomegaly, encephalopathy, cardiac failure
- Optic atrophy, cataracts, nystagmus, failure to fix and follow
- Appearance of external genitalia (micropenis)
- Midline defects (cleft lip, cleft palate, bifid uvula)
- Skin pigmentation (gums, scars, skin creases)
- Hemihypertrophy, macroglossia, omphalocoele
Causes of Hypoglycaemia
- Hypoglycaemia arises from an imbalance between glucose production and consumption and can be caused by either endocrine or metabolic disorders or may be secondary to other disorders or organ dysfunction.
Endocrine |
Hyperinsulinism Adrenal insufficiency Hypopituitarism Growth hormone deficiency Hypothyroidism (very rarely) Insulinoma (rare) |
Metabolic |
Fat oxidation defects Defects of ketone metabolism Glycogen storage diseases Defects of gluconeogenesis Disorders of organic acid metabolism |
Other |
Sepsis Idiopathic ketotic hypoglycaemia Drug related: insulin, sulphonlylureas, ethanol, methanol, salicylates, beta blockers, chemotherapy Liver failure Malaria |
Investigations
Clinical practice point
A key clinical practice point is to take blood and next urine for ketones at the time of hypoglycaemia and before treatment with glucose. The presence or absence of ketones at the time of hypoglycaemia is diagnostically crucial to aid diagnosis and subsequent management.
A key clinical practice point is to take blood and next urine for ketones at the time of hypoglycaemia and before treatment with glucose. The presence or absence of ketones at the time of hypoglycaemia is diagnostically crucial to aid diagnosis and subsequent management.
ALWAYS request laboratory serum glucose even if a finger prick glucose has been taken.
- Laboratory measurement for glucose is essential as point of care testing can be unreliable at low blood glucose levels.
ALWAYS contact biochemistry to inform them that samples are to be sent; SOME TESTS NEED TO REACH THE LAB URGENTLY FOR ANALYSIS.
- It is important to collect and save blood when the infant is hypoglycaemic for any specialist tests which may be subsequently required.
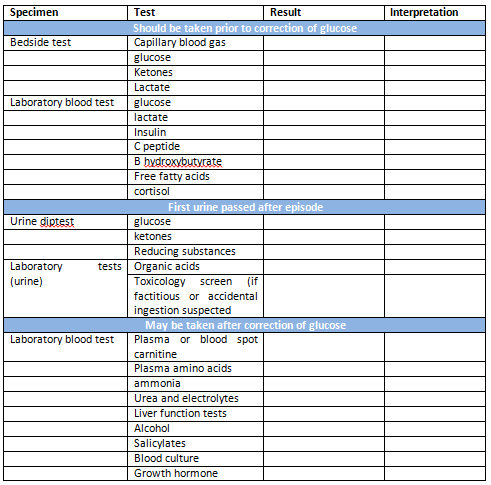
Time critical investigations
If sampling is difficult, the most important tests to collect at the time of hypoglycaemia are:
- Blood glucose
- Ketone level (request B-hydroxybutyrate)
- Blood gas
- Insulin level
- C-Peptide
- Cortisol
- Lactate
- 1st Urine passed
- Point of care testing for B hydroxybutyrate is now widely available.
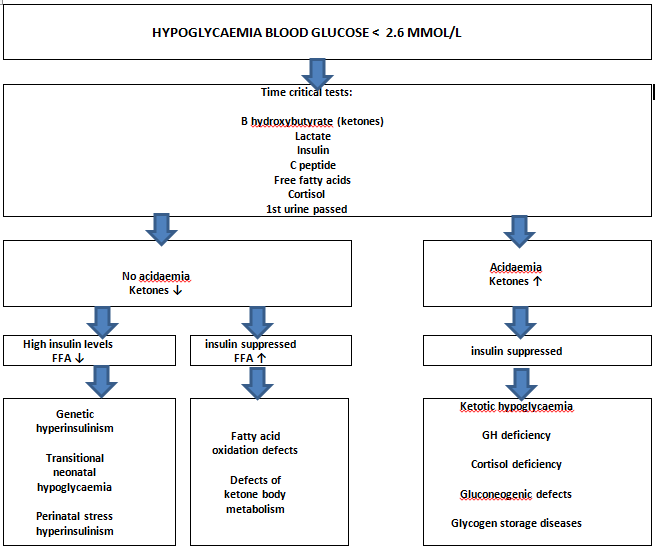
- Major categories of hypoglycaemia can be determined simply from analysis of a blood gas and ketone levels at the time of hypoglycaemia. This can help tailor any subsequent investigations.
- Hypoglycaemia with inappropriately low or absent ketones usually indicates hyperinsulinism as the underlying cause with the exception of fatty acid oxidation defects and defects of ketone metabolism.
Clinical practice point
A key practice point for interpreting the results of a hypoglycaemia screen is to interpret the episode of hypoglycaemia in the presence or absence of ketones and acidaemia.
This is diagnostically crucial to aid diagnosis and subsequent management and reinforces the need to take the appropriate time critical samples.
A key practice point for interpreting the results of a hypoglycaemia screen is to interpret the episode of hypoglycaemia in the presence or absence of ketones and acidaemia.
This is diagnostically crucial to aid diagnosis and subsequent management and reinforces the need to take the appropriate time critical samples.
Flow Chart
Investigations Required for a Complete Hypoglycaemia Screen
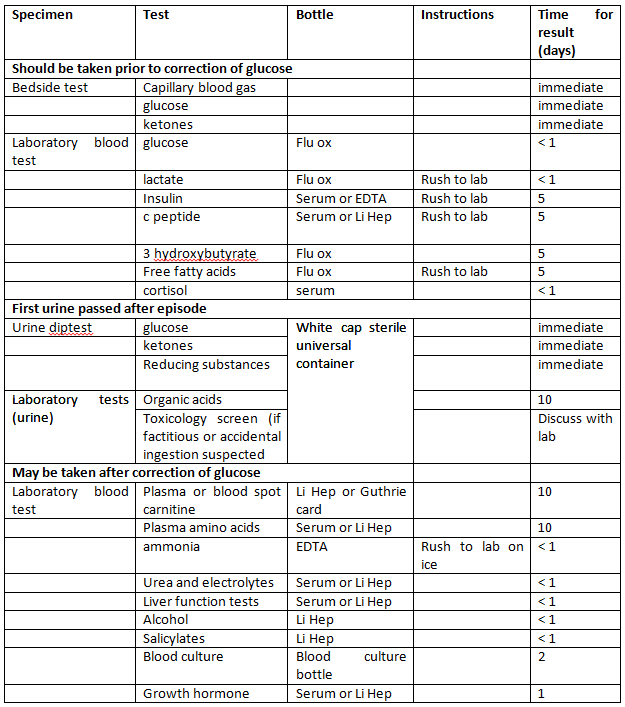
Bottles required:
Note: Bottles required for samples may vary slightly between laboratories
Turnaround time may be longer if transport to the laboratory is required
Hypoglycaemia: Grab bag/emergency box
Some units will have pre made emergency hypo boxes available in ED or on the paediatric wards which will include the bottles required for a hypoglycaemia screen.
- 2 x 2ml flu ox
- 2 x 2ml EDTA
- 6 x 2ml Li Hep
- Plain universal bottle 25 ml (10 mls urine)
Note: Bottles required for samples may vary slightly between laboratories
Turnaround time may be longer if transport to the laboratory is required
Hypoglycaemia: Grab bag/emergency box
Some units will have pre made emergency hypo boxes available in ED or on the paediatric wards which will include the bottles required for a hypoglycaemia screen.
Clinical practice point
If hypoglycaemia is though to the presenting feature of adrenal insufficiency, please see the following PIER guideline - Adrenal Crisis (new presentation or pre-existing adrenal insufficiency)
If hypoglycaemia is though to the presenting feature of adrenal insufficiency, please see the following PIER guideline - Adrenal Crisis (new presentation or pre-existing adrenal insufficiency)
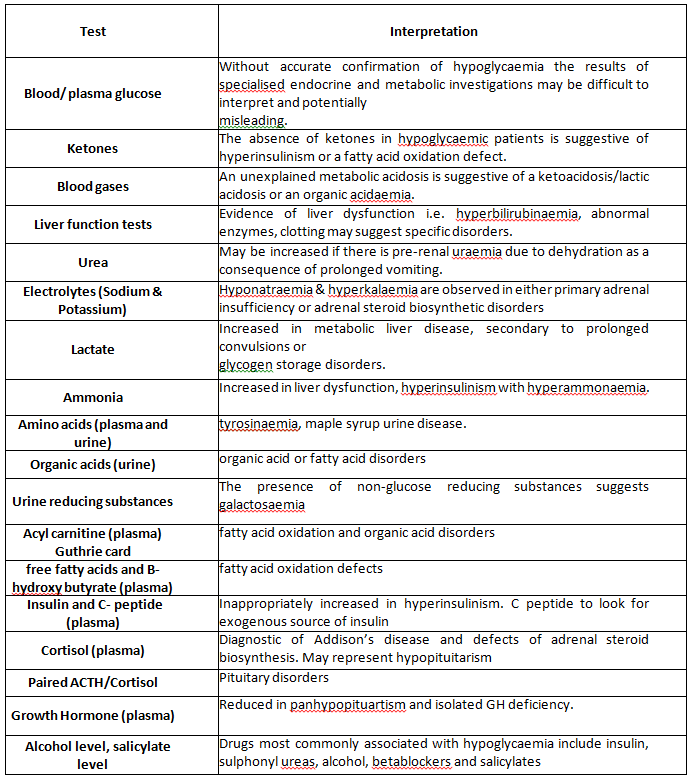
Interpretation of Hypoglycaemia Screening Tests
Controlled fasts
- Children who present with hypoglycaemia and have not had investigations carried out at the time of hypoglycaemia may require a controlled fast to help make a diagnosis.
- This is potentially dangerous and must be performed according to strict protocol in the hospital setting and should be discussed with the local DGH lead for endocrinology or tertiary centre at Southampton.
- It is important to exclude fatty acid oxidation defects and hyperinsulinism before subjecting a child to a controlled fast.
- Suspected adrenal insufficiency should be assessed by a short synacthen test prior to the fast.
Management of Hypoglycaemia
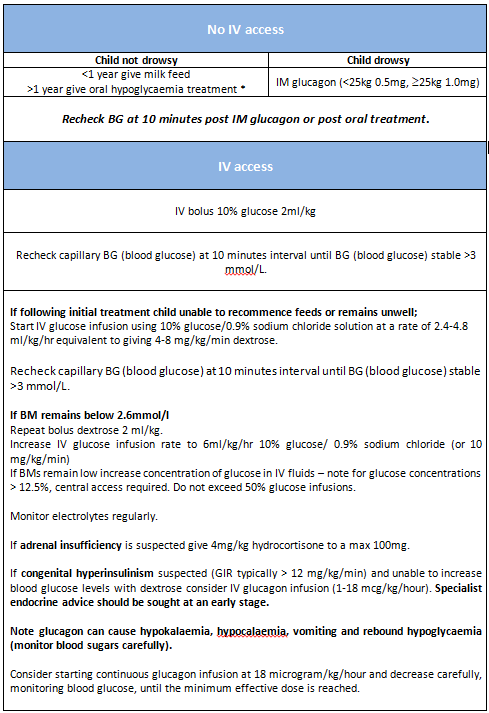
The correction of hypoglycaemia should follow standard practice guidelines (APLS) using intravenous glucose, glucagon injection or oral glucose (in the non-drowsy conscious patient).
DO NOT DELAY TREATMENT WHILST AWAITING CONFIRMATION OF LAB GLUCOSE
The correction of hypoglycaemia should follow standard practice guidelines (APLS) using intravenous glucose, glucagon injection or oral glucose (in the non-drowsy conscious patient).
- Assess patient using ABC framework
- Confirm Blood sugar < 2.6 mmol/l
- Insert IV cannula
- Take blood tests for hypoglycaemia screen
- Ensure lab glucose sent to confirm hypoglycaemia
- Put urine bag on to collect next urine passed
DO NOT DELAY TREATMENT WHILST AWAITING CONFIRMATION OF LAB GLUCOSE
See SORT guidelines for preparation of non-standard isotonic glucose concentrations and for glucose delivery calculations.
Blood glucose treatment targets
Treatment targets for blood glucose levels are aimed at avoiding activation of neuro endocrine responses and hypoglycaemia – associated autonomic failure (HAAF).
For children and adults with diabetes, neonates with a confirmed hypoglycaemia disorder and infants and children with a persistent hypoglycaemia disorder blood glucose levels should be kept above 3.9 mmol/l.
Glucose Infusion Rate (GIR)
The glucose infusion rate (mg/kg/min) can be calculated using the following formulae:
Blood glucose treatment targets
Treatment targets for blood glucose levels are aimed at avoiding activation of neuro endocrine responses and hypoglycaemia – associated autonomic failure (HAAF).
For children and adults with diabetes, neonates with a confirmed hypoglycaemia disorder and infants and children with a persistent hypoglycaemia disorder blood glucose levels should be kept above 3.9 mmol/l.
Glucose Infusion Rate (GIR)
- Calculating the amount of glucose required (glucose infusion rate, GIR) to maintain normoglycaemia is helpful when considering the diagnosis.
- Most infants will be normoglycaemic on an initial GIR of 5 – 8 mg/kg/min.
- Infants who are hyperinsulinaemic or have minimal glycogen stores may need a higher glucose infusion rate than 5 – 8 mg/kg/min to maintain normoglycaemia.
- Infants with congenital hyperinsulinism usually require a GIR greater than 12 mg/kg/min.
The glucose infusion rate (mg/kg/min) can be calculated using the following formulae:
GIR = % of glucose being infused x rate of infusion (ml/hr)/ Body weight (in kg) x 6
or
GIR = Rate of IV fluids (in ml/kg/day) x % of glucose infused/144
or
GIR = Rate of IV fluids (in ml/kg/day) x % of glucose infused x 0.007
or
GIR = Rate of IV fluids (in ml/kg/day) x % of glucose infused/144
or
GIR = Rate of IV fluids (in ml/kg/day) x % of glucose infused x 0.007
Oral hypoglycaemia treatment options
5-20g of fast acting oral carbohydrate should be given (approx. 0.3g/kg) see table below:
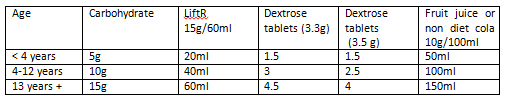
Chocolate or milk WILL NOT bring glucose levels up quickly enough
(Note Lucozade Sport (300ml = 20g))
IV Glucagon infusion preparation
SINGLE STRENGTH infusion
Add 1 mL of diluent provided (water) to the 1 mg vial (1000 microgram of glucagon). Draw up 0.5 mL/kg (0.5 mg/kg of glucagon) and make up to a final volume of 50 mL with glucose 5% or 0.9% sodium chloride to give a concentration of 10 microgram/kg/mL.
Infusing at 1 mL/hour = 10 microgram/kg/hour.
DOUBLE STRENGTH infusion
Add 1 mL of diluent provided (water) to the 1 mg vial (1000 microgram of glucagon). Draw up 1 mL/kg (1 mg/kg of glucagon) and make up to a final volume of 50 mL with glucose 5% or 0.9% sodium chloride with a concentration of 20 microgram/kg/mL.
Infusing at 1 mL/hour = 20 microgram/kg/hour.
(Note Lucozade Sport (300ml = 20g))
IV Glucagon infusion preparation
SINGLE STRENGTH infusion
Add 1 mL of diluent provided (water) to the 1 mg vial (1000 microgram of glucagon). Draw up 0.5 mL/kg (0.5 mg/kg of glucagon) and make up to a final volume of 50 mL with glucose 5% or 0.9% sodium chloride to give a concentration of 10 microgram/kg/mL.
Infusing at 1 mL/hour = 10 microgram/kg/hour.
DOUBLE STRENGTH infusion
Add 1 mL of diluent provided (water) to the 1 mg vial (1000 microgram of glucagon). Draw up 1 mL/kg (1 mg/kg of glucagon) and make up to a final volume of 50 mL with glucose 5% or 0.9% sodium chloride with a concentration of 20 microgram/kg/mL.
Infusing at 1 mL/hour = 20 microgram/kg/hour.
Discharge Planning
- It is important that a cause for the hypoglycaemia is established before the patient is discharged home and appropriate treatment and follow up plans arranged.
- If hypoglycaemia unexplained or at risk of hypoglycaemia, prior to discharge:
- Determine how long the child can safely remain normoglycaemic (see below)
- arrange open access to the ward
- train parents in monitoring blood sugars and treating hypoglycaemia
- arrange follow-up appointment
- A reasonable time between meals or feeds should be safely tolerated without blood sugar dropping below 3.0mmol/l. A controlled fast may be required and this should be discussed with the local DGH endocrine lead or tertiary centre.
- The details of treatment for specific conditions is beyond the scope of this guideline but may include involvement of the paediatric dietitians, training on hypoglycaemia management, home glucose monitoring and open access arrangements to the local centre.
Governance
Implementation
The guideline will be displayed on the PIER website and can be accessed by all healthcare professionals working within Wessex. This guideline will be disseminated to network centre leads within the Wessex Paediatric Endocrine Network.
Process for Monitoring Effectiveness
Compliance with the guideline will be audited and results disseminated to the Wessex Paediatric Endocrine Network. A service evaluation of parental satisfaction of initial management will be undertaken.
Implementation
The guideline will be displayed on the PIER website and can be accessed by all healthcare professionals working within Wessex. This guideline will be disseminated to network centre leads within the Wessex Paediatric Endocrine Network.
Process for Monitoring Effectiveness
Compliance with the guideline will be audited and results disseminated to the Wessex Paediatric Endocrine Network. A service evaluation of parental satisfaction of initial management will be undertaken.
Appendix
Hypoglycaemia Results Log - Print and File in Patient Notes
Hypoglycaemia Results Log - Print and File in Patient Notes
References
- APLS Manual 6e 2016.
- Southampton Oxford Retrieval Team guidelines SORT: https://www.sort.nhs.uk/Media/Guidelines/Glucose-concentrations-and-calculator.pdf
- BNFc, BNF.NICE.org.uk
- Medusa Injectable medicines guide: Glucagon, Version 6 published 07/12/2018
- ISPAD Clinical Practice Consensus Guidelines 2014. Assessment and management of hypoglycemia in children and adolescents with diabetes. Ly TT et al Pediatr Diabetes. 2014 Sep;15 Suppl 20:180-92. doi: 10.1111/pedi.12174. Epub 2014 Jul 12.
- ACDC clinical guideline: Management of hypoglycaemia in children with Type 1 diabetes 2016.
- Recognition, assessment and management of hypoglycaemia in childhood. Ghosh A, Banerjee I, Morris AAM, Arch Dis Child 2016; 101:575-580
- What is normal blood glucose? Güemes M, Rahman SA, Hussain K. Arch Dis Child 2016; 101: 569–574.
- Recommendations from the Paediatric Endocrine Society for Evaluation and Management of Persistent Hypoglycaemia in Neonates, Infants and Children. Thornton PS et al. The Journal of Paediatrics 2015, 167(2), May 2015
- How to use a controlled fast to investigate hypoglycaemia. Streekantam S, Preece MA, Vijay S et al Arc Dis Child Educ Pract Ed 2017; 102:28-36
- Investigation of the child with acute metabolic disorder. Cook P, Walker V. J Clin Pathol 2011; 64:181-191.
- Re-evaluating “Transitional Neonatal Hypoglycaemia”: Mechanism and implications for management. Stanley CA. J Pediatr. 2015 June; 166(6): 1520–5.
|
Document Version:
1.0 Lead Author: Dr Eleri Williams, Paediatric Consultant |
Approving Network:
Wessex Paediatric Endocrine Network Date of Approval: 08/2023 Review Date: 08/2026 |
PIER Contact |
|