The Use of Haemopoietic Growth Factors in Paediatric Oncology and Haematology Patients
Introduction
This guideline has been produced to make recommendations for the use of Granulocyte Colony Stimulating Factors (GCSF) in paediatric patients undergoing chemotherapy for cancer. This document aims to combine up to date research, current thinking, and local expert opinion to generate Network Guidelines.
This guideline has been produced to make recommendations for the use of Granulocyte Colony Stimulating Factors (GCSF) in paediatric patients undergoing chemotherapy for cancer. This document aims to combine up to date research, current thinking, and local expert opinion to generate Network Guidelines.
Scope and Purpose
This guideline applies to all paediatric oncology patients who require haematopoietic growth factors for supportive care of cancer treatment.
The purpose of the guideline is
This guideline applies to all paediatric oncology patients who require haematopoietic growth factors for supportive care of cancer treatment.
The purpose of the guideline is
- To provide background information relating to indications of haematopoietic growth factors
- To provide support for the prescribing and supplying of appropriate formulations of Granulocyte- Colony Stimulating Factors (G-CSF)
Definitions
G-CSF Granulocye Colony Stimulating Factor
PBSC Peripheral Blood Stem Cells
CLS Capillary Leak Syndrome
PTC Principal Treatment Centre
G-CSF Granulocye Colony Stimulating Factor
PBSC Peripheral Blood Stem Cells
CLS Capillary Leak Syndrome
PTC Principal Treatment Centre
Background
Recombinant human granulocyte-colony stimulating factor (rhG-CSF) stimulates the production of neutrophils and may reduce the duration of chemotherapy induced neutropenia.
Bone marrow suppression is among the most common toxicities encountered as a result of chemotherapeutic treatment of malignancy. In addition to life-threatening complications arising from neutropenia, thrombocytopenia and anaemia, dose reductions and dose delays may compromise treatment outcomes
Recombinant human granulocyte-colony stimulating factor (rhG-CSF) stimulates the production of neutrophils and may reduce the duration of chemotherapy induced neutropenia.
Bone marrow suppression is among the most common toxicities encountered as a result of chemotherapeutic treatment of malignancy. In addition to life-threatening complications arising from neutropenia, thrombocytopenia and anaemia, dose reductions and dose delays may compromise treatment outcomes
Indications
Primary prophylaxis and treatment
GCSF can be used for prolonged neutropenia and within those patients who are at higher risk of infectious complications, when it is not necessarily recommended within the treatment protocol.
Consider primary prophylaxis in patients who have:
Secondary prophylaxis
Secondary prophylaxis can be initiated in between chemotherapy cycles after an occurrence of chemotherapy induced prolonged neutropenia or febrile neutropenia, with or without dose delay, in a setting where clinical data supports the maintenance of dose intensity or the requirement to avoid chemotherapy delays.
Use of GCSF in Progenitor Stem Cell Transplantation
The three most commonly used mobilisation regimens at Southampton Children’s Hospital are:
Primary prophylaxis and treatment
GCSF can be used for prolonged neutropenia and within those patients who are at higher risk of infectious complications, when it is not necessarily recommended within the treatment protocol.
Consider primary prophylaxis in patients who have:
- Extensive prior chemotherapy
- Previous irradiation to the pelvis or other areas containing large amounts of bone marrow
- Conditions that potentially enhance the risk of serious infection.
- The protocol recommends the use of GCSF to maintain treatment intensity (e.g. rapid COJEC).
Secondary prophylaxis
Secondary prophylaxis can be initiated in between chemotherapy cycles after an occurrence of chemotherapy induced prolonged neutropenia or febrile neutropenia, with or without dose delay, in a setting where clinical data supports the maintenance of dose intensity or the requirement to avoid chemotherapy delays.
Use of GCSF in Progenitor Stem Cell Transplantation
- Mobilisation of peripheral blood stem cells (PBSC)
The three most commonly used mobilisation regimens at Southampton Children’s Hospital are:
- GCSF alone
- Cyclophosphamide with GCSF
- GCSF and plerixafor.
- Post PBSC reinfusion
Dose and Administration
Initiation
GCSF should not be administered within 24 hours of cytotoxic chemotherapy- therefore start at least 24 hours after the completion of chemotherapy and stop at least 24 hours before next chemotherapy due.
The only exception to this is subsequent boluses of vincristine etc administered on day 8 or day 15 of a cycle.
Duration
The duration of treatment will be documented on the patients discharge summary and may also be in the treatment protocol. For patients receiving GCSF after myelosuppressive therapy, the duration of treatment will often depend on their white cell or neutrophil count. GCSF should not be stopped before the nadir. The nadir usually occurs 7-10 days after the start of chemotherapy. If the patient’s white cell count rises significantly before the nadir, discuss this with the PTC team. GCSF is often continued for a minimum of 7 days and until neutrophils > 1 x 109/L for 2 or 3 consecutive days after the nadir.
The platelet count is useful to identify when the nadir has passed, as the platelet count will begin to rise, and is unaffected by GCSF.
For patients receiving GCSF prior to a stem cell harvest, omitting or stopping the GCSF will significantly affect their stem cell mobilisation. Please discuss with PTC.
For patients due chemotherapy, GCSF should be stopped at least 24 hours before the planned start date of chemotherapy.
Patients with high risk neuroblastoma, during rapid COJEC will receive GCSF as per specific regimen as stated in the protocol. Chemotherapy is administered at 10 day intervals and GCSF is given as primary prophylaxis for 6-7 days in between, to ensure the patient can receive the scheduled chemotherapy on time and to minimise gut toxicity. Please refer to the high risk neuroblastoma protocol for the GCSF schedule.
Monitoring
The frequency of blood tests required will be communicated on the patients discharge summary. As a rough guide, children on GCSF will require a full blood count (FBC) at least twice per week.
For patients due to receive count-dependent chemotherapy, a FBC will need to be taken at least 48 hours after the last dose of GCSF. This is in order to accurately assess the patient’s own bone marrow recovery.
Formulation
Filgrastim is available at UHS as:
Filgrastim is a biological medicine and must be prescribed and dispensed by brand name.
Note: 1million units of filgrastim solution for injection is equivalent to 10micrograms of filgrastim.
Filgrastim
1st line for the treatment and prophylaxis of chemotherapy induced neutropenia
Standard Dose: 5mcg/kg (max. 300mcg) OD SC
Doses < 120mcg or for parents who may struggle to manipulate the prefilled syringes:
Doses may be manufactured in a Pharmacy Aseptic Unit using the Neupogen® 300mcg/ml vials. Doses manufactured in an unlicensed unit will have an expiry of 7 days maximum and must be stored in the refrigerator. Round doses to the nearest 0.05ml (nearest 15mcg).
Initiation
GCSF should not be administered within 24 hours of cytotoxic chemotherapy- therefore start at least 24 hours after the completion of chemotherapy and stop at least 24 hours before next chemotherapy due.
The only exception to this is subsequent boluses of vincristine etc administered on day 8 or day 15 of a cycle.
Duration
The duration of treatment will be documented on the patients discharge summary and may also be in the treatment protocol. For patients receiving GCSF after myelosuppressive therapy, the duration of treatment will often depend on their white cell or neutrophil count. GCSF should not be stopped before the nadir. The nadir usually occurs 7-10 days after the start of chemotherapy. If the patient’s white cell count rises significantly before the nadir, discuss this with the PTC team. GCSF is often continued for a minimum of 7 days and until neutrophils > 1 x 109/L for 2 or 3 consecutive days after the nadir.
The platelet count is useful to identify when the nadir has passed, as the platelet count will begin to rise, and is unaffected by GCSF.
For patients receiving GCSF prior to a stem cell harvest, omitting or stopping the GCSF will significantly affect their stem cell mobilisation. Please discuss with PTC.
For patients due chemotherapy, GCSF should be stopped at least 24 hours before the planned start date of chemotherapy.
Patients with high risk neuroblastoma, during rapid COJEC will receive GCSF as per specific regimen as stated in the protocol. Chemotherapy is administered at 10 day intervals and GCSF is given as primary prophylaxis for 6-7 days in between, to ensure the patient can receive the scheduled chemotherapy on time and to minimise gut toxicity. Please refer to the high risk neuroblastoma protocol for the GCSF schedule.
Monitoring
The frequency of blood tests required will be communicated on the patients discharge summary. As a rough guide, children on GCSF will require a full blood count (FBC) at least twice per week.
For patients due to receive count-dependent chemotherapy, a FBC will need to be taken at least 48 hours after the last dose of GCSF. This is in order to accurately assess the patient’s own bone marrow recovery.
Formulation
Filgrastim is available at UHS as:
- Neupogen® 300microgram/ml vial
- Biosimilar filgrastim Accofil 300mcg/0.5ml prefilled syringe for subcutaneous injection
- Pegfilgrastim or Lipegfilgrastim prefilled 6mg syringe for subcutaneous injection (peglated formulation, given as a stat dose: Only funded for sarcoma patients).
Filgrastim is a biological medicine and must be prescribed and dispensed by brand name.
Note: 1million units of filgrastim solution for injection is equivalent to 10micrograms of filgrastim.
Filgrastim
1st line for the treatment and prophylaxis of chemotherapy induced neutropenia
Standard Dose: 5mcg/kg (max. 300mcg) OD SC
Doses < 120mcg or for parents who may struggle to manipulate the prefilled syringes:
Doses may be manufactured in a Pharmacy Aseptic Unit using the Neupogen® 300mcg/ml vials. Doses manufactured in an unlicensed unit will have an expiry of 7 days maximum and must be stored in the refrigerator. Round doses to the nearest 0.05ml (nearest 15mcg).
Weight (kg) |
Filgrastim Dose |
< 6kg |
Consult Pharmacist |
6-7 kg |
30 mcg |
8-10 kg |
45 mcg |
11-13 kg |
60 mcg |
14-16 kg |
75 mcg |
17-19 kg |
90 mcg |
20-22 kg |
105 mcg |
Doses ≥ 120mcg
Accofil (Filgrastim Biosimilar) 300mcg/0.5ml prefilled syringes with graduations at 15mcg (0.025ml) may be used.
These prefilled syringes have a longer expiry than the in-house manufactured product.
Syringes should be stored in the refrigerator, however may be removed from the refrigerator and left at room temperature (not above 25°C) for a single period (that ends before the labelled expiry date) for up to 15 days.
Accofil (Filgrastim Biosimilar) 300mcg/0.5ml prefilled syringes with graduations at 15mcg (0.025ml) may be used.
These prefilled syringes have a longer expiry than the in-house manufactured product.
Syringes should be stored in the refrigerator, however may be removed from the refrigerator and left at room temperature (not above 25°C) for a single period (that ends before the labelled expiry date) for up to 15 days.
Weight (kg) |
Dose (mcg) |
Volume of Accofil 300mcg/0.5ml (ml) |
23 - 26 kg |
120 mcg |
0.2 ml |
27 - 28 kg |
135 mcg |
0.225 ml |
29 - 32 kg |
150 mcg |
0.25 ml |
33 - 34 kg |
165 mcg |
0.275 ml |
35 - 38 kg |
180 mcg |
0.3 ml |
39 - 40 kg |
195 mcg |
0.325 ml |
41 - 43 kg |
210 mcg |
0.35 ml |
44 - 46 kg |
225 mcg |
0.375 ml |
47 - 49 kg |
240 mcg |
0.4 ml |
50 - 51 kg |
255 mcg |
0.425 ml |
53 - 55 kg |
270 mcg |
0.45 ml |
56 - 58 kg |
285 mcg |
0.475 ml |
59 - 60 kg |
300 mcg |
0.5 ml |
Please note that two strengths of Accofil pre-filled syringes are available – 300mcg/0.5ml and 480mcg/0.5ml – ensure the patient is dispensed the correct strength. If a patient, parent or carer struggles to manipulate the pre-filled syringe (i.e. expelling unnecessary liquid), doses can be manufactured in an aseptic unit as described above.
Pre harvest dose: 10microgram/kg SC OD (IV route is not to be used for this indication).
For patients weighing <12kg or parents unable to manipulate 300mcg/0.5ml prefilled syringe
Doses may be manufactured in a Pharmacy Aseptic Unit using the 300mcg/ml vials. Doses manufactured in an unlicensed unit will have an expiry of 7 days maximum and must be stored in the refrigerator. Round doses to the nearest 0.05ml (nearest 15mcg).
For patients weighing >12kg to 30kg
Accofil (Filgrastim Biosimilar) 300mcg/0.5ml prefilled syringes with graduations at 15mcg (0.025ml) may be used.
These prefilled syringes have a longer expiry than the in-house manufactured product.
Syringes should be stored in the refrigerator, however may be removed from the refrigerator and left at room temperature (not above 25°C) for a single period (that ends before the labelled expiry date) of up to 15 days.
Pre harvest dose: 10microgram/kg SC OD (IV route is not to be used for this indication).
For patients weighing <12kg or parents unable to manipulate 300mcg/0.5ml prefilled syringe
Doses may be manufactured in a Pharmacy Aseptic Unit using the 300mcg/ml vials. Doses manufactured in an unlicensed unit will have an expiry of 7 days maximum and must be stored in the refrigerator. Round doses to the nearest 0.05ml (nearest 15mcg).
For patients weighing >12kg to 30kg
Accofil (Filgrastim Biosimilar) 300mcg/0.5ml prefilled syringes with graduations at 15mcg (0.025ml) may be used.
These prefilled syringes have a longer expiry than the in-house manufactured product.
Syringes should be stored in the refrigerator, however may be removed from the refrigerator and left at room temperature (not above 25°C) for a single period (that ends before the labelled expiry date) of up to 15 days.
Weight (kg) |
Filgrastim (biosimilar brand) dose (mcg) |
Volume of Accofil 300mcg/0.5ml (ml) |
12 kg |
120 mcg |
0.2 ml |
13 - 14 kg |
135 mcg |
0.225 ml |
15 kg |
150 mcg |
0.25 ml |
16 - 17 kg |
165 mcg |
0.275 ml |
18 kg |
180 mcg |
0.3 ml |
19 - 20 kg |
195 mcg |
0.325 ml |
21 kg |
210 mcg |
0.35 ml |
22 - 23 kg |
225 mcg |
0.375 ml |
24 kg |
240 mcg |
0.4 ml |
25 - 26 kg |
255 mcg |
0.425 ml |
27 kg |
270 mcg |
0.45 ml |
28 - 29 kg |
285 mcg |
0.475 ml |
30 kg |
300 mcg |
0.5 ml |
For patients weighing >30kg, the below dosing schedule is recommended.
Weight (kg) |
Filgrastim (biosimilar brand) dose (mcg) |
Prefilled syringes used |
30 - 39 kg |
300 mcg |
1 x 300 mcg |
40 - 54 kg |
480 mcg |
1 x 480 mcg |
55 - 68 kg |
600 mcg |
2 x 300 mcg |
69 - 87 kg |
780 mcg |
1 x 300 mcg + 1 x 480 mcg |
> 88 kg |
960 mcg |
2 x 480 mcg |
Route and dilution
As a subcutaneous (SC) bolus – give undiluted.
An insuflon™ may be used for the administration of subcutaneous GCSF.
An insulflon™ must not be used for GCSF given prior to a stem cell harvest. A proportion of the dose remains in the lumen of the insuflon™, and it is imperative prior to stem cell harvest, that patients receive the full dose.
An insuflon™ may be left in situ for maximum 7 days, changed sooner if soiled or becomes unstuck. Do not flush the insuflon.
The dose of GCSF can be removed from the refrigerator 30 minutes before injection to reduce local irritation or stinging.
As an intravenous infusion over 30 minutes (not to be given IV before harvest)
As a subcutaneous (SC) bolus – give undiluted.
An insuflon™ may be used for the administration of subcutaneous GCSF.
An insulflon™ must not be used for GCSF given prior to a stem cell harvest. A proportion of the dose remains in the lumen of the insuflon™, and it is imperative prior to stem cell harvest, that patients receive the full dose.
An insuflon™ may be left in situ for maximum 7 days, changed sooner if soiled or becomes unstuck. Do not flush the insuflon.
The dose of GCSF can be removed from the refrigerator 30 minutes before injection to reduce local irritation or stinging.
As an intravenous infusion over 30 minutes (not to be given IV before harvest)
- Doses manufactured in an aseptic unit can be ordered for IV infusion and will be ready diluted for infusion.
- The prefilled syringes can also be diluted for IV infusion by a healthcare professional, in 5% dextrose to a final concentration greater than 15microgram/mL
- Flush infusion with 5% dextrose.
- Not compatible with sodium chloride solutions
Parental GCSF Competency
If parents or carers are to be administering the subcutaneous doses of GCSF whilst the patient is at home, the parents/carers must be trained and deemed competent before discharge. To aid teaching, please refer to the Parental GCSF competency document, which includes a declaration of competence assessed by a nurse and parent/carer for both direct injection and injection via insuflon™.
If parents or carers are to be administering the subcutaneous doses of GCSF whilst the patient is at home, the parents/carers must be trained and deemed competent before discharge. To aid teaching, please refer to the Parental GCSF competency document, which includes a declaration of competence assessed by a nurse and parent/carer for both direct injection and injection via insuflon™.
PEGFilgrastim (Neulasta)
Funded only for sarcoma patients.
Dose: 100microgram/kg (max. 6mg) SC 24-48hrs post the completion of chemotherapy.
Prefilled syringes are not graduated and are spring loaded; therefore if the dose is less than 6mg, the dose must be withdrawn from the syringe by a healthcare professional. This is unlicensed. PEGFilgrastim doses may only be manipulated by the local hospital.
Funded only for sarcoma patients.
Dose: 100microgram/kg (max. 6mg) SC 24-48hrs post the completion of chemotherapy.
Prefilled syringes are not graduated and are spring loaded; therefore if the dose is less than 6mg, the dose must be withdrawn from the syringe by a healthcare professional. This is unlicensed. PEGFilgrastim doses may only be manipulated by the local hospital.
Adverse Effects
GCSF is usually well tolerated; occasionally, localised reactions may be observed at the injection site. Other common side effects include nausea and vomiting and bone pain.
Musculoskeletal pain and headaches may be experienced, and patients should be warned of these effects.
Other side effects are rare but may include transient hypotension, thrombocytopenia, disturbances in liver enzymes and serum uric acid, splenic enlargement.
Spleen size should be monitored during treatment – risk of splenomegaly and rupture.
GCSF is usually well tolerated; occasionally, localised reactions may be observed at the injection site. Other common side effects include nausea and vomiting and bone pain.
Musculoskeletal pain and headaches may be experienced, and patients should be warned of these effects.
Other side effects are rare but may include transient hypotension, thrombocytopenia, disturbances in liver enzymes and serum uric acid, splenic enlargement.
Spleen size should be monitored during treatment – risk of splenomegaly and rupture.
MHRA alert: Filgrastim and PegFilgrastim: Risk of Capillary Leak Syndrome (CLS) - December 2014
A review of filgrastim and pegfilgrastim was triggered by postmarketing reports of capillary leak syndrome (CLS). CLS is characterised by:
Advice for healthcare professionals: (September 2013).
Closely monitor all patients and healthy donors for CLS symptoms, which commonly have rapid onset. Symptoms include:
Advise patients and healthy donors to contact their doctor immediately if they develop CLS symptoms
Any suspected adverse reactions to filgrastim or pegfilgrastim should be reported to the MHRA using the Yellow Card scheme.
A review of filgrastim and pegfilgrastim was triggered by postmarketing reports of capillary leak syndrome (CLS). CLS is characterised by:
- hypotension and oedema
- hypoalbuminaemia
- haemoconcentration
Advice for healthcare professionals: (September 2013).
Closely monitor all patients and healthy donors for CLS symptoms, which commonly have rapid onset. Symptoms include:
- generalised body swelling
- puffiness (which may be associated with less-frequent urination)
- difficulty breathing; abdominal swelling
- tiredness
Advise patients and healthy donors to contact their doctor immediately if they develop CLS symptoms
Any suspected adverse reactions to filgrastim or pegfilgrastim should be reported to the MHRA using the Yellow Card scheme.
Implementation
This guideline will be disseminated across the Wessex Paediatric Cancer Network
This guideline will be disseminated across the Wessex Paediatric Cancer Network
Process for Monitoring Effectiveness
Reduced variation in practice has been shown to improve outcomes. Please detail how the impact of this guideline will be measured to demonstrate its effectiveness and identify areas for further development. Where possible this should include patient reported outcomes.
Reduced variation in practice has been shown to improve outcomes. Please detail how the impact of this guideline will be measured to demonstrate its effectiveness and identify areas for further development. Where possible this should include patient reported outcomes.
References
- Neupogen 30MU (0.3mg/ml) solution for injection SPC. Last updated 2/08/18, Accessed on 25/4/19. Available at https://www.medicines.org.uk/emc/product/3000/smpc
- Accofil 30MU/0.5ML (0.6MG/ML) solution for injection or infusion SPC. Last updated 16/02/19, Accessed on 25/4/19. Available at https://www.medicines.org.uk/emc/product/3384
- https://www.gov.uk/drug-safety-update/filgrastim-and-pegfilgrastim-risk-of-capillary-leak-syndrome
- http://www.londoncancer.org/media/78165/London-Cancer-GCSF-Guidelines-v1.pdf
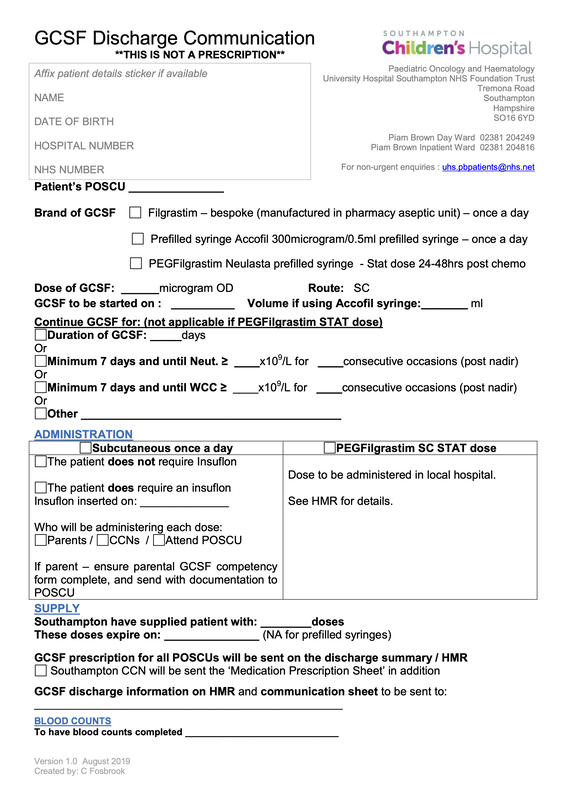
Appendix A: GCSF Discharge Communication Sheet
(Click to download)
(Click to download)
Appendix B: Email Address Contacts for POSCUS
POSCU |
Email address and telephone contact |
Basingstoke and Winchester |
|
Chichester |
|
Dorchester |
|
Frimley |
|
Guernsey |
|
Isle of Wight |
[email protected] 01983 534690 |
Jersey |
[email protected] 01534 442122 |
Poole |
[email protected] CCN: 01202 448279 |
Portsmouth |
[email protected] 023 9228 6602 |
Salisbury |
[email protected] CCN: 07976 857855 or 07976 857789 |
Southampton CCN |
[email protected] 023 8054 0031 |
Worthing |
|
Document Version:
1.0 Lead Authors: C Fosbrook, Paediatric Oncology Pharmacist H Blundell, Clinical Facilitator |
Approving Network:
Paediatric Oncology Date of Approval: September 2023 Review Date: September 2026 |
PIER Contact |
|