Management of raised neonatal bloodspot TSH and initial management of congenital hypothyroidism
Flowchart
Introduction
Untreated severe congenital hypothyroidism can lead to neurological and psychiatric deficits including intellectual disability, spasticity, and disturbances of gait and co-ordination.
Congenital hypothyroidism is one of the most common preventable causes of mental retardation. Newborn screening programmes have been successful in the early detection of infants with congenital hypothyroidism. Early institution of levothyroxine treatment can eliminate the severe neurodevelopmental deficits which will occur if there is a late diagnosis or delayed treatment with thyroxine.
Untreated severe congenital hypothyroidism can lead to neurological and psychiatric deficits including intellectual disability, spasticity, and disturbances of gait and co-ordination.
Congenital hypothyroidism is one of the most common preventable causes of mental retardation. Newborn screening programmes have been successful in the early detection of infants with congenital hypothyroidism. Early institution of levothyroxine treatment can eliminate the severe neurodevelopmental deficits which will occur if there is a late diagnosis or delayed treatment with thyroxine.
Scope
Paediatricians working in DGHs across Wessex, and consultants covering when the designated lead for paediatric endocrinology at each DGH is on leave.
Each DGH across the Wessex Paediatric Endocrine Network has a designated lead for the management of babies with congenital hypothyroidism (please see Wessex Paediatric Endocrine Network) and to whom the newborn screening laboratory will ring positive results. If this individual is away, there will be alternative local arrangements in place to enable prompt action of a newborn screening positive result (usually consultant of the week).
Paediatricians working in DGHs across Wessex, and consultants covering when the designated lead for paediatric endocrinology at each DGH is on leave.
Each DGH across the Wessex Paediatric Endocrine Network has a designated lead for the management of babies with congenital hypothyroidism (please see Wessex Paediatric Endocrine Network) and to whom the newborn screening laboratory will ring positive results. If this individual is away, there will be alternative local arrangements in place to enable prompt action of a newborn screening positive result (usually consultant of the week).
Purpose
The aim of the guideline is to improve patient experience, clinical outcomes, provide an agreed clinical approach to managing these babies, enable prompt institution of levothyroxine with no delay and optimise communication with parents.
The aim of the guideline is to improve patient experience, clinical outcomes, provide an agreed clinical approach to managing these babies, enable prompt institution of levothyroxine with no delay and optimise communication with parents.
Definitions
Newborn screening of blood TSH can detect primary congenital hypothyroidism. This condition causes an elevated blood TSH with a low or normal FT4 and results from either thyroid agenesis (thyroid gland absent or ectopically sited) or from dyshormonogenesis (thyroid gland present but an enzymatic defect leads to abnormally low thyroid hormone synthesis).
Secondary hypothyroidism (which may occur from congenital abnormalities of the hypothalamic-pituitary axis) will result in a normal or low TSH with a low FT4 and will not be detected by the newborn TSH screen.
CHT - Congenital Hypothyroidism
TSH - Thyroid Stimulating Hormone
Newborn screening of blood TSH can detect primary congenital hypothyroidism. This condition causes an elevated blood TSH with a low or normal FT4 and results from either thyroid agenesis (thyroid gland absent or ectopically sited) or from dyshormonogenesis (thyroid gland present but an enzymatic defect leads to abnormally low thyroid hormone synthesis).
Secondary hypothyroidism (which may occur from congenital abnormalities of the hypothalamic-pituitary axis) will result in a normal or low TSH with a low FT4 and will not be detected by the newborn TSH screen.
CHT - Congenital Hypothyroidism
TSH - Thyroid Stimulating Hormone
Important points to guide the history and examination
Important points to guide the history
Enquire about:
Important points to guide the examination
Important points to guide the history
Enquire about:
- Family history of thyroid disease
- Maternal history of thyroid disease (including past history of thyroidectomy)
- Medication taken during pregnancy (including anti-thyroid drugs-carbimazole, PTU)
- Baby
- reduced/slow feeding,
- sleepiness, not waking for feeds,
- jaundice
- any supplements containing biotin given to baby
Important points to guide the examination
- goitre or posterior lingual swelling
- check for congenital abnormalities (especially cardiac)
- underlying dysmorphic syndromes
- jaundice
- hypotonia
- umbilical hernia
- dry skin
- document head circumference
Investigations required following an elevated TSH result confirmed by newborn screening
Baby
Mother
Baby
- TSH.
- FT4.
- FT3
- Thyroglobulin (a marker of the presence of thyroid tissue).
Mother
- TSH.
- Free T4.
- Thyroid TPO antibodies .
Biochemical criteria used in the decision to start treatment
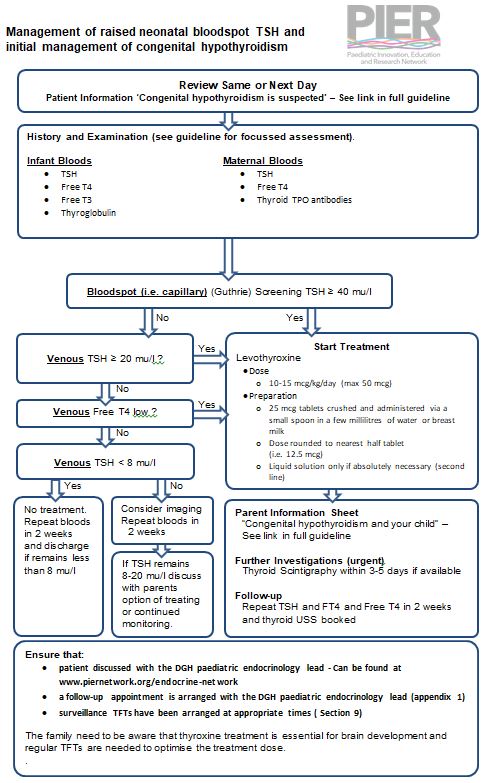
- If capillary TSH concentration from blood obtained on neonatal screening is ≥ 40 mu/L whole blood (this is the result which is phoned through from the newborn screening laboratory)
- start treatment as soon as a good venous sample for a TSH and FT4 can be obtained, and without waiting for the venous blood result (unless venous TFT results are available on the same day)
- If capillary TSH concentration from blood obtained on neonatal screening is ≤ 40Mu/L whole blood (this is the result which is phoned through from the newborn screening laboratory)
- the clinician may wait for results of the venous TFT (TSH and FT4) provided that these results are available the following day
Decision to start treatment on the basis of the venous TFTs (TSH and FT4)
- if the venous FT4 concentration is below the normal range for age, treatment should be started immediately
- if the venous TSH > 20mU/L, treatment should be started even if FT4 is normal
- if the venous TSH concentration is 8-20 mu/L beyond 21 days in a well baby with a FT4 concentration within the limits for age the baby requires investigation (thyroid imaging) and consideration of commencing levothyroxine and re-testing off treatment at a later stage
- give patient information leaflet to parents: Public Health England 'Congenital Hypothyroidism is suspected'
Thyroid Imaging
- Imaging should never delay the initiation of thyroxine treatment
- If levothyroxine is commenced, the baby should have a thyroid USS (this can be done as a routine investigation and following commencement of thyroxine)
- a thyroid uptake scan (radioisotope) should be organised, if available, and undertaken within 5 days of starting thyroxine
Follow Up of babies with an elevated TSH result
- These babies should be followed up by the DGH lead for paediatric endocrinology at each hospital in Wessex (please see Wessex Paediatric Endocrine Network)
Initial treatment of babies with congenital hypothyroidism
- The baby should be seen the same day or within 24 hours of the result being called through
- Levothyroxine should be initiated immediately after confirmatory bloods test results are available
- The initial starting dose is 10-15 microgrammes/Kg per day given orally
- Infants with severe disease (very low FT4) should be treated with 15 microgrammes/Kg per day
- Levothyroxine tablets should be crushed and administered using a small spoon, in a few millilitres of water or breast milk (do not dissolve in a bottle of milk as the powder will stick to the inside of the bottle resulting in inadequate dosing)
- Levothyroxine liquid should only be used if pharmaceutically (licenced) produced (tablets are the preferred preparation)
- Parents should be provided with written instruction on levothyroxine treatment
Discharge Planning
- Ensure that parents:
- Understand the reasons for the need for excellent medicine adherence
- Have been shown how to administer levothyroxine
- have been given a patient information leaflet; "congenital hypothyroidism is suspected"
- have been informed of date of next blood test and where to go
- have been informed of the timings of the TFT surveillance required (next section)
- thyroid imaging booked
- follow-up appointment booked with the local lead for paediatric endocrinology at relevant DGH
Monitoring of babies and children with congenital hypothyroidism treated with levothyroxine
*Clinical practice point
The interpretation of the TFT following 2 weeks of levothyroxine treatment is to confirm that the FT4 is in the normal range. The TSH may not have returned to normal but should be lower than at diagnosis. If there is no improvement check parental understanding of medicine administration, whether the importance medicine adherence is understood or whether there are other issues.
More frequent evaluations should be undertaken if compliance is questioned or abnormal values are obtained. Failure to comply with treatment must be addressed urgently and may be a safeguarding issue.
Clinical practice point
Steady state TSH levels are usually achieved after 4 consecutive weeks on the same dose of levothyroxine.
Therefore the time interval between TFTs to check whether a dose adjustment of levothyroxine is required should be 4 weeks (not earlier), so that a decision can be made whether or not the levothyroxine dose should change.
Any levothyroxine dose changes are usually in steps of 12.5 micrograms (i.e. half tablet)
- TSH concentrations should be maintained in the age-specific reference range
- FT4 concentrations should be maintained in the upper half of the age-specific reference range
- The first follow-up examination should take place 1-2 weeks after treatment with levothyroxine
- Repeat TFT (TSH and FT4) should be taken on the following weeks after starting levothyroxine:
- 2 weeks*
- 4 weeks
- 8 weeks
- 12 weeks
*Clinical practice point
The interpretation of the TFT following 2 weeks of levothyroxine treatment is to confirm that the FT4 is in the normal range. The TSH may not have returned to normal but should be lower than at diagnosis. If there is no improvement check parental understanding of medicine administration, whether the importance medicine adherence is understood or whether there are other issues.
More frequent evaluations should be undertaken if compliance is questioned or abnormal values are obtained. Failure to comply with treatment must be addressed urgently and may be a safeguarding issue.
Clinical practice point
Steady state TSH levels are usually achieved after 4 consecutive weeks on the same dose of levothyroxine.
Therefore the time interval between TFTs to check whether a dose adjustment of levothyroxine is required should be 4 weeks (not earlier), so that a decision can be made whether or not the levothyroxine dose should change.
Any levothyroxine dose changes are usually in steps of 12.5 micrograms (i.e. half tablet)
Follow Up frequency after three months of age
- 0-1 years: 1-3 monthly
- 1-4 years: 2-4 monthly
- > 4 years: 3-12 monthly
Factors that may lead to elevated TSH whilst on levothyroxine treatment
- Under-dosed with thyroxine
- Incorrect drug administration
- Medicine non-adherence
- Gastrointestinal problems, malabsorption
- Use of:
- soy milk
- infacol
- soy milk
- Interaction with the following medications:
- calcium supplements or treatment
- iron
- antacids, omeprazole
- tannins (from tea)
- supplements containing biotin
- enzyme inducing drugs: carbamazepine, phenytoin
- heparin
- amiodarone
- calcium supplements or treatment
- Assay interference (discuss with biochemist for a TFT assessment by alternative laboratory)
Implementation
- `The guideline will be displayed on the PIER website and can be accessed by all healthcare professionals working within Wessex. This guideline will be disseminated to network centre leads within the Wessex Paediatric Endocrine Network. Treatment of congenital hypothyroidism will be managed locally by the paediatric endocrinology network lead at each DGH (details here).
Process for Monitoring Effectiveness
- Effectiveness of the guideline will be monitored by feedback to the lead author.
Patient Information Leaflets
- Patient Information Leaflets from Public Health England:
References
- Leger J, Olivieri A, Donaldson M, et al. European Society for Paediatric Endocrinology consensus guidelines on screening, diagnosis, and management of congenital hypothyroidism. J Clin Endocrinol Metab 2014;99:363–84.
- Congenital hypothyroidism: initial clinical referral standards and guidelines. UK Newborn Screening Programme Centre, 2013
- https://www.gov.uk/government/publications/congenital-hypothyroidism-screening-laboratory-handbook
- UK standards for Paediatric Endocrinology, BSPED & RCPCH, 2019 https://www.bsped.org.uk/media/1580/uk-standards-for-paediatric-endocrinology-2019.pdf
- Burch HB. Drug Effects on the Thyroid. N Engl J Med 2019;381:749-61
|
Document Version:
1.2 Lead Author: Dr Justin Davis, Paediatric Endocrinology Consultant |
Approving Network:
Wessex Paediatric Endocrine Network Date of Approval: 05/2024 Review Date: 05/2027 |
PIER Contact |
|