The Assessment and Management of Overweight and Obesity in Children and Young People
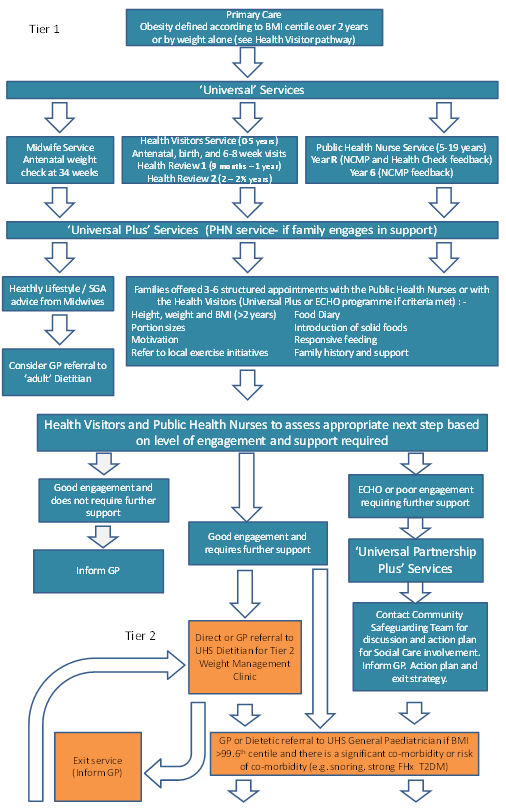
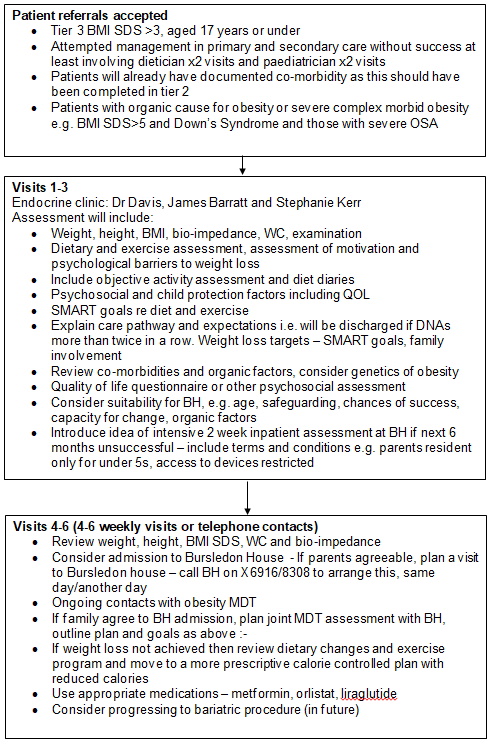
Flowchart: Paediatric Obesity Care Pathway 2018
Scope and Purpose
Currently this guideline is only intended for Southampton services as regional services vary widely around Hampshire. We will continue to accept tertiary referrals from regional secondary care paediatricians if the appropriate co-morbidity screening has been done and there is a significant co-morbidity – see flow chart above.
Purpose of guideline:
Currently this guideline is only intended for Southampton services as regional services vary widely around Hampshire. We will continue to accept tertiary referrals from regional secondary care paediatricians if the appropriate co-morbidity screening has been done and there is a significant co-morbidity – see flow chart above.
Purpose of guideline:
- To set referral criteria according to NICE guidance and current capacity
- To support assessment of paediatric obesity in secondary care
- To support management in secondary and tertiary care
- To clarify movement of patients between tiers 1-4
- To provide guidance and education for all UHS staff to be able to manage paediatric obesity
- To ensure management of children and young people is in line with current guidelines and recommendations and is evidence based.
Background
Overweight and obesity in children is becoming more widespread in the UK with reports that 1 in 3 children aged 2-15 are now overweight (1). Children are becoming overweight earlier and staying overweight for longer (2). Children from poorer backgrounds are twice as likely to be overweight or obese at five years old and this is increased to three times as likely by the time they are eleven years old (3). The full extent of the long term effects of this is not known, but the metabolic changes that result are known to lead to type 2 diabetes, metabolic syndrome, cardiovascular disease, cancer and mental illness. These can be linked directly to overweight and obesity, and it is more important than ever that a strategy to prevent obesity is in place in the wider community. For those children who are already overweight and obese, robust support is needed.
It is within this context that a tier 3 service for patients with established obesity and significant co-morbidities, and a tier 2 service for patients requiring dietetic support to help prevent their progression in co-morbidities and worsening obesity, have been set up.
The major role of tier 2 is to assess and initiate management of those with significant obesity. Assessment should involve an exclusion of an organic cause, assessment of co-morbidity, assessment of diet, exercise and psychosocial factors including motivation, eating behaviour, quality of life and safeguarding issues. Management requires consistency between health professionals in tier 2 and tier 3 and includes recommendations regarding diet and exercise, SMART goals, self monitoring and supporting behavioural change.
Overweight and obesity in children is becoming more widespread in the UK with reports that 1 in 3 children aged 2-15 are now overweight (1). Children are becoming overweight earlier and staying overweight for longer (2). Children from poorer backgrounds are twice as likely to be overweight or obese at five years old and this is increased to three times as likely by the time they are eleven years old (3). The full extent of the long term effects of this is not known, but the metabolic changes that result are known to lead to type 2 diabetes, metabolic syndrome, cardiovascular disease, cancer and mental illness. These can be linked directly to overweight and obesity, and it is more important than ever that a strategy to prevent obesity is in place in the wider community. For those children who are already overweight and obese, robust support is needed.
It is within this context that a tier 3 service for patients with established obesity and significant co-morbidities, and a tier 2 service for patients requiring dietetic support to help prevent their progression in co-morbidities and worsening obesity, have been set up.
The major role of tier 2 is to assess and initiate management of those with significant obesity. Assessment should involve an exclusion of an organic cause, assessment of co-morbidity, assessment of diet, exercise and psychosocial factors including motivation, eating behaviour, quality of life and safeguarding issues. Management requires consistency between health professionals in tier 2 and tier 3 and includes recommendations regarding diet and exercise, SMART goals, self monitoring and supporting behavioural change.
Definitions & Diagnosis
According to NICE, the definition of overweight is a BMI percentile > 91st percentile and the definition of obesity is a BMI percentile > 98th percentile. However co-morbidities are much higher in the group with BMI > 99.6th percentile or > 3 standard deviation scores (SDS). These cut off points are a useful tool, but do not give the full picture. Other factors such as a family history of type 2 diabetes can indicate a greater risk of developing metabolic complications including diabetes, high blood pressure and raised blood lipids. Ethnicity is also a factor, and patients of Asian origin might require a lower threshold for the definition of overweight and obesity. Conversely patients of black African or Caribbean origin may require a higher threshold. Pubertal patients have a much higher risk of metabolic co-morbidities.
Diagnosis of overweight or obesity would normally occur in primary care. The National Child Measurement Programme (NCMP) letter is a tool used by public health nurses to inform parents of the overweight or obesity status of their child. Initiatives to engage children and families exist, such as ‘change for life’ internet-based resources. Local areas also have access to alternative programmes, such as that run by the Hampshire Fire Service. The public health nurses are best placed to signpost parents to the local diet and lifestyle programmes that exist in a particular area.
According to NICE, the definition of overweight is a BMI percentile > 91st percentile and the definition of obesity is a BMI percentile > 98th percentile. However co-morbidities are much higher in the group with BMI > 99.6th percentile or > 3 standard deviation scores (SDS). These cut off points are a useful tool, but do not give the full picture. Other factors such as a family history of type 2 diabetes can indicate a greater risk of developing metabolic complications including diabetes, high blood pressure and raised blood lipids. Ethnicity is also a factor, and patients of Asian origin might require a lower threshold for the definition of overweight and obesity. Conversely patients of black African or Caribbean origin may require a higher threshold. Pubertal patients have a much higher risk of metabolic co-morbidities.
Diagnosis of overweight or obesity would normally occur in primary care. The National Child Measurement Programme (NCMP) letter is a tool used by public health nurses to inform parents of the overweight or obesity status of their child. Initiatives to engage children and families exist, such as ‘change for life’ internet-based resources. Local areas also have access to alternative programmes, such as that run by the Hampshire Fire Service. The public health nurses are best placed to signpost parents to the local diet and lifestyle programmes that exist in a particular area.
Care Pathway Tier 2
Public health nurses, GPs, and health visitors can refer patients to the tier 2 dietetic led obesity service led by the UHS paediatric endocrine dietetic team if the following criteria are fulfilled:
Children under 2 years:
Baby’s weight is > 99.6th centile before 6 months of age if they were > 50th centile at birth
OR if they have crossed more than 3 centiles upwards in 6 months
Children over 2 yrs:
BMI > 99.6th centile
OR BMI > 98th centile with significant co-morbidities
OR BMI > 98th centile and this has not reduced over 6 months despite support and increased monitoring
Clinics will be held at the Royal South Hants Hospital (RSH) weekly.
Obese patients who have risk of developing co-morbidities will require further screening by a tier 2 General Paediatrician (currently Dr Sarah Williams and Dr Mark Alderton) to document co-morbidity and to exclude organic causes such as obesity syndromes and endocrinopathy.
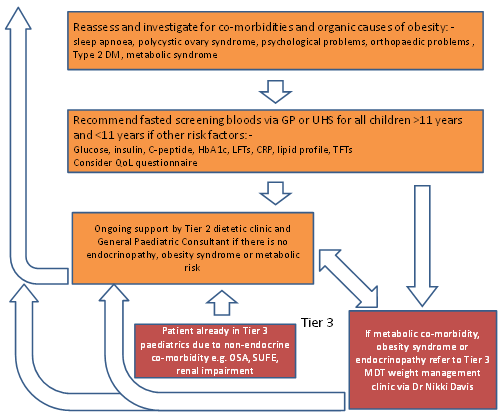
If they have an endocrine or metabolic co-morbidity they may as a result of this be referred to the tier 3 obesity multidisciplinary clinic led by Dr Nikki Davis held weekly. Some of these patients may also been seen in the weekly general endocrine clinic.
Obese patients with a non-endocrine co-morbidity such as SUFE, hypertension, OSA should be managed the Paediatrician leading for this co-morbidity with the support of the tier 2 dietetic team (to be developed into MDT) and also using resources from primary care when applicable (e.g. MEND). There will be some exceptions to this if the obesity or co-morbidity is very severe and requires more specialist input via Dr Davis and the tier 3 MDT.
Ideally over time the tier 2 and tier 3 services will be extended and developed so that they can be more effective (and cost-effective) and can increase capacity. In the future the tier 2 MDT in weight management should include a dietician, specialist nurse, physiotherapist and psychologist and a link to social care, and could be overseen by a general paediatrician with an interest in obesity.
Tier 3 consultants seeing patients with co-morbidities of obesity e.g. renal, respiratory, orthopaedic and hepatology consultants can also access the tier 2 weight management MDT via referral to the General Paediatricians with an interest in obesity (currently Dr Sarah Williams and Dr Mark Alderton).
Patients from primary care can be referred in to these services via these General Paediatricians as long as the BMI SDS score is > 3 i.e. the BMI is > 99.6th percentile. Patients can stay in the tier 2 weight management MDT for up to 2 years before discharge back to primary care weight management services.
Exit criteria have been developed but may need adjustment according to future capacity. For the tier 2 service, children who are WNB for more than one appointment can be discharged to primary care if there are no active safeguarding concerns and no co-morbidity. If safeguarding concerns exist e.g. significant harm from co-morbidity, then children’s services may need to be involved to ensure future engagement with medical services. Those who engage and actively lose weight can be discharged when their BMI SDS is < 98th percentile or when the co-morbidity has resolved. Many young people however will require long term support with weight management and this will need to be assessed on an individual basis.
The tier 3 service currently comprises Dr Nikki Davis, specialist dieticians (James Barratt) and a specialist nurse (Stephanie Kerr). In the future, service development will aim to expand the MDT according to NICE guidance to also add input from a physiotherapist, psychologist and a link to social care but would be overseen by Dr Nikki Davis. These children should all have a documented endocrine co-morbidity such as metabolic syndrome, obesity syndrome, or PCOS. Obesity is such a major problem in the health service at the moment that there is a need to attempt to concentrate resources on those who are able to change their lifestyle and achieve healthier weights in the long term. In the Tier 3 service we offer 2 years of engagement with the MDT weight management service. Discharge can be before 2 years if there is poor engagement or poor attendance and there are no safeguarding or significant harm concerns. However, it is less likely that these patients can be discharged if WNB, due to the presence of significant co-morbidity which may require safeguarding or Children’s service support. Some young people will need long term support with weight management if they have complex needs and co-morbidity.
Public health nurses, GPs, and health visitors can refer patients to the tier 2 dietetic led obesity service led by the UHS paediatric endocrine dietetic team if the following criteria are fulfilled:
Children under 2 years:
Baby’s weight is > 99.6th centile before 6 months of age if they were > 50th centile at birth
OR if they have crossed more than 3 centiles upwards in 6 months
Children over 2 yrs:
BMI > 99.6th centile
OR BMI > 98th centile with significant co-morbidities
OR BMI > 98th centile and this has not reduced over 6 months despite support and increased monitoring
Clinics will be held at the Royal South Hants Hospital (RSH) weekly.
Obese patients who have risk of developing co-morbidities will require further screening by a tier 2 General Paediatrician (currently Dr Sarah Williams and Dr Mark Alderton) to document co-morbidity and to exclude organic causes such as obesity syndromes and endocrinopathy.
If they have an endocrine or metabolic co-morbidity they may as a result of this be referred to the tier 3 obesity multidisciplinary clinic led by Dr Nikki Davis held weekly. Some of these patients may also been seen in the weekly general endocrine clinic.
Obese patients with a non-endocrine co-morbidity such as SUFE, hypertension, OSA should be managed the Paediatrician leading for this co-morbidity with the support of the tier 2 dietetic team (to be developed into MDT) and also using resources from primary care when applicable (e.g. MEND). There will be some exceptions to this if the obesity or co-morbidity is very severe and requires more specialist input via Dr Davis and the tier 3 MDT.
Ideally over time the tier 2 and tier 3 services will be extended and developed so that they can be more effective (and cost-effective) and can increase capacity. In the future the tier 2 MDT in weight management should include a dietician, specialist nurse, physiotherapist and psychologist and a link to social care, and could be overseen by a general paediatrician with an interest in obesity.
Tier 3 consultants seeing patients with co-morbidities of obesity e.g. renal, respiratory, orthopaedic and hepatology consultants can also access the tier 2 weight management MDT via referral to the General Paediatricians with an interest in obesity (currently Dr Sarah Williams and Dr Mark Alderton).
Patients from primary care can be referred in to these services via these General Paediatricians as long as the BMI SDS score is > 3 i.e. the BMI is > 99.6th percentile. Patients can stay in the tier 2 weight management MDT for up to 2 years before discharge back to primary care weight management services.
Exit criteria have been developed but may need adjustment according to future capacity. For the tier 2 service, children who are WNB for more than one appointment can be discharged to primary care if there are no active safeguarding concerns and no co-morbidity. If safeguarding concerns exist e.g. significant harm from co-morbidity, then children’s services may need to be involved to ensure future engagement with medical services. Those who engage and actively lose weight can be discharged when their BMI SDS is < 98th percentile or when the co-morbidity has resolved. Many young people however will require long term support with weight management and this will need to be assessed on an individual basis.
The tier 3 service currently comprises Dr Nikki Davis, specialist dieticians (James Barratt) and a specialist nurse (Stephanie Kerr). In the future, service development will aim to expand the MDT according to NICE guidance to also add input from a physiotherapist, psychologist and a link to social care but would be overseen by Dr Nikki Davis. These children should all have a documented endocrine co-morbidity such as metabolic syndrome, obesity syndrome, or PCOS. Obesity is such a major problem in the health service at the moment that there is a need to attempt to concentrate resources on those who are able to change their lifestyle and achieve healthier weights in the long term. In the Tier 3 service we offer 2 years of engagement with the MDT weight management service. Discharge can be before 2 years if there is poor engagement or poor attendance and there are no safeguarding or significant harm concerns. However, it is less likely that these patients can be discharged if WNB, due to the presence of significant co-morbidity which may require safeguarding or Children’s service support. Some young people will need long term support with weight management if they have complex needs and co-morbidity.
Tier 2 Assessment for Paediatric Obesity
Assessment for organic causes of morbid obesity
The vast majority of children with obesity have ‘simple obesity’ or ‘environmental obesity’ i.e. there is no underlying cause for the obesity- obesity is due to a sustained positive energy balance due to taking in more calories than they are using.
There are a number of organic causes of obesity:
This is a short guide to an initial assessment to be done in secondary care Paediatrics to help exclude organic causes of obesity and is based on the following principles.
Endocrinopathies are nearly always associated with short stature and include GHD, Cushing’s disease, pituitary disease, hypothalamic disease, hypothyroidism, and pseudohypoparathyroidism types 1A and B (Albright’s hereditary osteodystrophy).
Syndromic conditions are nearly always obvious and include developmental delay, dysmorphic features, renal abnormalities, deafness and visual problems.
Non-syndromic but genetic conditions causing obesity all have a pattern of early onset (during infancy) weight gain and hyperphagia. These are rare but include leptin deficiency, MC4R mutations and a host of other rare conditions currently emerging from genetic studies.
Iatrogenic causes include chemotherapy, radiotherapy and steroid use. Hypothalamic and cranial tumours can also cause obesity but again the history here is usually very obvious. Children who have had total body irradiation for bone marrow transplant and those with craniopharyngiomas are particularly severely affected.
In summary, if the child is of normal height (usually in the upper part of the mid-parental target range), has normal height velocity, has normal development and no other obvious syndromic features or history of congenital hyperphagia, it is extremely unlikely that there is an organic cause for obesity.
Important points in the medical history
Co-morbidities of obesity
Examination for obesity
Investigations and interpretation
Signs of endocrine disease
Obesity syndromes
Consider if there are any dysmorphic features or developmental abnormalities.
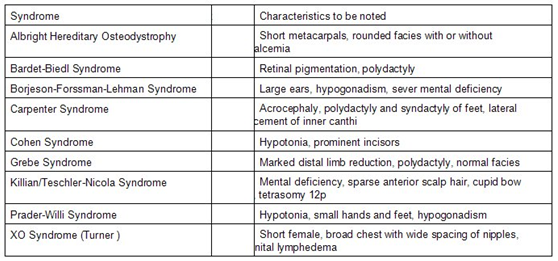
Table 1: Common short stature obesity genetic syndromes
Assessment for organic causes of morbid obesity
The vast majority of children with obesity have ‘simple obesity’ or ‘environmental obesity’ i.e. there is no underlying cause for the obesity- obesity is due to a sustained positive energy balance due to taking in more calories than they are using.
There are a number of organic causes of obesity:
- Endocrinopathies
- Syndromic conditions
- Non-syndromic conditions with congenital hyperphagia
- Iatrogenic including late effects after childhood cancer
This is a short guide to an initial assessment to be done in secondary care Paediatrics to help exclude organic causes of obesity and is based on the following principles.
Endocrinopathies are nearly always associated with short stature and include GHD, Cushing’s disease, pituitary disease, hypothalamic disease, hypothyroidism, and pseudohypoparathyroidism types 1A and B (Albright’s hereditary osteodystrophy).
Syndromic conditions are nearly always obvious and include developmental delay, dysmorphic features, renal abnormalities, deafness and visual problems.
Non-syndromic but genetic conditions causing obesity all have a pattern of early onset (during infancy) weight gain and hyperphagia. These are rare but include leptin deficiency, MC4R mutations and a host of other rare conditions currently emerging from genetic studies.
Iatrogenic causes include chemotherapy, radiotherapy and steroid use. Hypothalamic and cranial tumours can also cause obesity but again the history here is usually very obvious. Children who have had total body irradiation for bone marrow transplant and those with craniopharyngiomas are particularly severely affected.
In summary, if the child is of normal height (usually in the upper part of the mid-parental target range), has normal height velocity, has normal development and no other obvious syndromic features or history of congenital hyperphagia, it is extremely unlikely that there is an organic cause for obesity.
Important points in the medical history
- Birth weight
- Growth
- Age of onset of obesity
- History of hyperphagia
- Waking at night demanding food/ go looking for food
- Demand more food immediately after a meal
- Eat rapidly and is not easily distracted from food
- Never feels full and can eat very large portions
- Development
- Pubertal development
- Family history
- Consanguineous family
- Early-onset obesity
- Diabetes, renal or cardiovascular disease
- Hyperphagia
- Co-morbidities
Co-morbidities of obesity
- Diabetes and metabolic syndrome
- NAFLD
- PCOS
- Cardiovascular disease
- Obstructive sleep apnoea
- Psychological problems
- Orthopaedic problems
- Social and educational exclusion
- Gallstones
- Cancers
- Worsening of other conditions e.g. renal disease
Examination for obesity
- Height, weight, Tanner stage, BMI SDS, waist circumference
- Pubertal stage (can be reported rather than formally examined)
- Blood pressure
- Acanthosis nigricans
- Hair colour
- Dysmorphic features
- Pattern of fat distribution: central versus peripheral
- Hearing and vision
Investigations and interpretation
- Fasted glucose, insulin, C-peptide, HbA1c, LFTs, CRP, lipid profile, TFTs
- OGTT if pubertal or post-pubertal with either acanthosis nigricans or high risk family history
- Genetics of obesity panel if relevant – see Appendix 1
- Definition of impaired fasted glucose > 5.6 - 6.9 mmol/l
- T2DM: fasted glucose > 6.9 mmol/l
- Fasting hyperinsulinaemia: insulin >10mu/l in pre-pubertal children and >20 mu/l in pubertal children
- HbA1c < 42mmo/mol is normal
- LFTs: raised ALT is likely to indicate NAFLD
- CRP 3-10 is an independent indicator of increased cardiovascular risk
- Lipid profile: dyslipidaemia is indicated by non-HDL > 3.6mmol/l, or LDL > 3.2mmol/l, or HDL< 0.9 mmol/l or triglycerides > 1.6mmol/l
- OGTT: Impaired glucose tolerance is defined as two-hour glucose levels of 7.8 to 11.0 mmol/l
Signs of endocrine disease
- Patient is short for parental target range or has poor height velocity as well as obesity. This includes the following conditions:
- Hypothalamic disease
- Late effects after brain tumour
- Narcolepsy
- Hypothalamic syndrome
- Growth hormone deficiency
- Hypothyroidism
- Cushing’s syndrome
- Steroid use
- Hypothalamic disease
Obesity syndromes
Consider if there are any dysmorphic features or developmental abnormalities.
Table 1: Common short stature obesity genetic syndromes
Known obesity genes
Most also have dysmorphic features and developmental problems. Also consider if the history is consistent with autosomal dominant congenital hyperphagia.
Appendix B shows the clinical assessment form which can help with consideration of a patient for a genetics of obesity gene panel (currently at East Anglia Medical Genetics Service, Addenbrookes, Cambridge)
Table 2: Obesity genes (4)
Most also have dysmorphic features and developmental problems. Also consider if the history is consistent with autosomal dominant congenital hyperphagia.
Appendix B shows the clinical assessment form which can help with consideration of a patient for a genetics of obesity gene panel (currently at East Anglia Medical Genetics Service, Addenbrookes, Cambridge)
Table 2: Obesity genes (4)

All Tiers - Management of Paediatric Obesity
Barriers to effective management
The main challenge with managing families with severe obesity is lack of engagement for a range of psychosocial factors. Commonly children in an obese family are not seen as obese by their parents because obesity is normal for them and now normal for the population. Families can feel criticised and judged. Many families are poorly resourced and struggling with economic, health and social challenges and obesity management is therefore not seen as a priority. There is often co-morbid depression, anxiety and low self esteem.
There is often a level of denial. People do not often appreciate how toxic obesity is when it starts in childhood. 30% the current cohort of children who remain slim are expected to live to 100 years old. However the same generation overall has a lower life expectancy than their parents due to obesity related early mortality (5). Obesity has a similar impact on life expectancy to smoking 20 cigarettes per day (6) and this is likely to be accelerated for those who are obese from childhood. Still most people believe it is a cosmetic issue and feel the medical services are overstating the risks (7).
Public Health England report that 600 million pounds was spent in 2016 promoting high sugar foods to children.
Unfortunately the food industry has no mandatory responsibility at present to address these problems. Food labelling is very confusing (e.g. the ‘Innocent’ smoothie). The average child in this country consumes twice the recommended daily amount of sugar before they leave the breakfast table and three times the recommended level over a whole day (8).
Eating outside of the home is increasing and as more parents work there is increased reliance on processed and fast foods with high levels of sugar, salt and trans- fats. Many people do not cook and falsely believe healthy food to be more expensive. Healthy eating behaviour is also disrupted by working hours.
Consultation style
Most parents engage more effectively with a non-judgemental approach whereby this is discussed as a health problem from the outset rather than a judgement on parenting. We are all living in a highly obesogenic society.
An initial thorough detailed assessment encourages engagement as it personalises the investigations and management plan. Most families require positive support and reinforcement that success is within their grasp. Frequent reviews are required to maintain motivation. Motivational interviewing can be very helpful as it encourages responsibility and self efficacy. Most information needs to be targeted to the family as a whole unit. For children less than 11 years the parents should be mainly in control of the diet provided to the child, whereas older children need to be supported and educated to make healthy choices independently when outside the home. Advice between different health professionals needs to be as consistent as possible.
Diet
Healthy eating is a good start for everyone. Most families think they are already following this but are not in reality. Diet diaries are essential in order to make recommendations and the vast majority of people will be unable to give a clear dietary history or have an idea of appropriate portioning.
Portion control is very important as obese people often lack satiety and have poor internal hunger signals. In childhood, insulin resistance drives hunger in order to drive growth, particularly during adolescence and this is physiological in normal weight adolescents. In an obese individual, high post-prandial insulin levels are pathologically sustained, and insulin resistance becomes excessive, driving hunger but also driving carbohydrate into fat storage. The insulin signalling also damages the hypothalamus which would normally signal satiety, and the child is hungry after consuming carbohydrates, which are laid down as fat and also is unable to feel full (9). This pattern of hunger is extremely common (10) and is one of the factors causing severe weight gain in puberty, particularly in girls and those who are inactive or have a family history of T2DM.
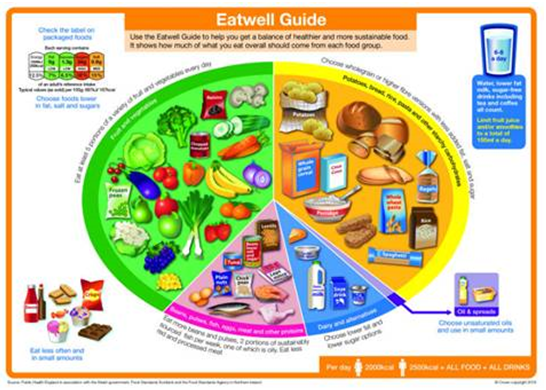
This pattern should be managed with a portion controlled low sugar and low glycaemic index diet. Slimming world is not portion controlled and so is not always appropriate for an obese adolescent. Many people think that the ‘five a day’ advice is always healthy. It is very common to meet children consuming 5 lots of high sugar fruits such as grapes and bananas and no vegetables. 3 portions of the ‘5 a day’ should be vegetables and 2 should be fruit. Only one portion a day should be juice or smoothie. Recommending the change4life website, the sugar smart app and the Eatwell guide can be very helpful.
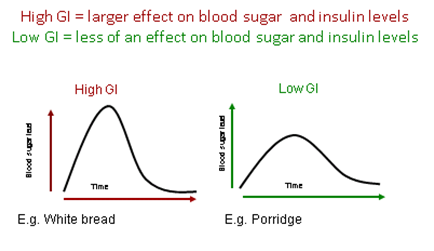
Glycaemic Index
The glycaemic index (GI) is a ranking of carbohydrates on a scale from 0 to 100 according to the extent to which they raise blood sugar and insulin levels after eating.
Barriers to effective management
The main challenge with managing families with severe obesity is lack of engagement for a range of psychosocial factors. Commonly children in an obese family are not seen as obese by their parents because obesity is normal for them and now normal for the population. Families can feel criticised and judged. Many families are poorly resourced and struggling with economic, health and social challenges and obesity management is therefore not seen as a priority. There is often co-morbid depression, anxiety and low self esteem.
There is often a level of denial. People do not often appreciate how toxic obesity is when it starts in childhood. 30% the current cohort of children who remain slim are expected to live to 100 years old. However the same generation overall has a lower life expectancy than their parents due to obesity related early mortality (5). Obesity has a similar impact on life expectancy to smoking 20 cigarettes per day (6) and this is likely to be accelerated for those who are obese from childhood. Still most people believe it is a cosmetic issue and feel the medical services are overstating the risks (7).
Public Health England report that 600 million pounds was spent in 2016 promoting high sugar foods to children.
Unfortunately the food industry has no mandatory responsibility at present to address these problems. Food labelling is very confusing (e.g. the ‘Innocent’ smoothie). The average child in this country consumes twice the recommended daily amount of sugar before they leave the breakfast table and three times the recommended level over a whole day (8).
Eating outside of the home is increasing and as more parents work there is increased reliance on processed and fast foods with high levels of sugar, salt and trans- fats. Many people do not cook and falsely believe healthy food to be more expensive. Healthy eating behaviour is also disrupted by working hours.
Consultation style
Most parents engage more effectively with a non-judgemental approach whereby this is discussed as a health problem from the outset rather than a judgement on parenting. We are all living in a highly obesogenic society.
An initial thorough detailed assessment encourages engagement as it personalises the investigations and management plan. Most families require positive support and reinforcement that success is within their grasp. Frequent reviews are required to maintain motivation. Motivational interviewing can be very helpful as it encourages responsibility and self efficacy. Most information needs to be targeted to the family as a whole unit. For children less than 11 years the parents should be mainly in control of the diet provided to the child, whereas older children need to be supported and educated to make healthy choices independently when outside the home. Advice between different health professionals needs to be as consistent as possible.
Diet
Healthy eating is a good start for everyone. Most families think they are already following this but are not in reality. Diet diaries are essential in order to make recommendations and the vast majority of people will be unable to give a clear dietary history or have an idea of appropriate portioning.
Portion control is very important as obese people often lack satiety and have poor internal hunger signals. In childhood, insulin resistance drives hunger in order to drive growth, particularly during adolescence and this is physiological in normal weight adolescents. In an obese individual, high post-prandial insulin levels are pathologically sustained, and insulin resistance becomes excessive, driving hunger but also driving carbohydrate into fat storage. The insulin signalling also damages the hypothalamus which would normally signal satiety, and the child is hungry after consuming carbohydrates, which are laid down as fat and also is unable to feel full (9). This pattern of hunger is extremely common (10) and is one of the factors causing severe weight gain in puberty, particularly in girls and those who are inactive or have a family history of T2DM.
This pattern should be managed with a portion controlled low sugar and low glycaemic index diet. Slimming world is not portion controlled and so is not always appropriate for an obese adolescent. Many people think that the ‘five a day’ advice is always healthy. It is very common to meet children consuming 5 lots of high sugar fruits such as grapes and bananas and no vegetables. 3 portions of the ‘5 a day’ should be vegetables and 2 should be fruit. Only one portion a day should be juice or smoothie. Recommending the change4life website, the sugar smart app and the Eatwell guide can be very helpful.
Glycaemic Index
The glycaemic index (GI) is a ranking of carbohydrates on a scale from 0 to 100 according to the extent to which they raise blood sugar and insulin levels after eating.
A healthy eating pattern for a child or young person should result in:
• 50-55% of their total energy (kilocalories) coming from carbohydrate
• Less than 35% of their total energy (kilocalories) from fat (with less than 10% of fat being saturated fat)
• 15-20% of their total energy (kilocalories) intake coming from protein.
There is lots of evidence to suggest that increasing the protein content of the diet moderately (to 30%) can improve satiety in young people. Extreme low carbohydrate diets (ketogenic) in children are not recommended for weight management as they can affect growth and cause adverse lipid profiles.
The Eatwell Guide
• 50-55% of their total energy (kilocalories) coming from carbohydrate
• Less than 35% of their total energy (kilocalories) from fat (with less than 10% of fat being saturated fat)
• 15-20% of their total energy (kilocalories) intake coming from protein.
There is lots of evidence to suggest that increasing the protein content of the diet moderately (to 30%) can improve satiety in young people. Extreme low carbohydrate diets (ketogenic) in children are not recommended for weight management as they can affect growth and cause adverse lipid profiles.
The Eatwell Guide
Estimated Average Energy Requirements
Table 3 shows the Estimated Average Requirement (EAR) for girls and boys aged 1 to 18 years (this is the total energy on average you would expect a healthy active child or adolescent to consume each day). It also shows how much carbohydrate (grams) would need to be eaten to provide the recommended 50-55% of the daily energy intake. For young people who are underweight, overweight or particularly active or inactive the recommended daily intake would be different. This information can offer some guidance and help establish a healthy eating pattern.
Table 3: EAR and suggested daily carbohydrate intake according to age and sex
Table 3 shows the Estimated Average Requirement (EAR) for girls and boys aged 1 to 18 years (this is the total energy on average you would expect a healthy active child or adolescent to consume each day). It also shows how much carbohydrate (grams) would need to be eaten to provide the recommended 50-55% of the daily energy intake. For young people who are underweight, overweight or particularly active or inactive the recommended daily intake would be different. This information can offer some guidance and help establish a healthy eating pattern.
Table 3: EAR and suggested daily carbohydrate intake according to age and sex
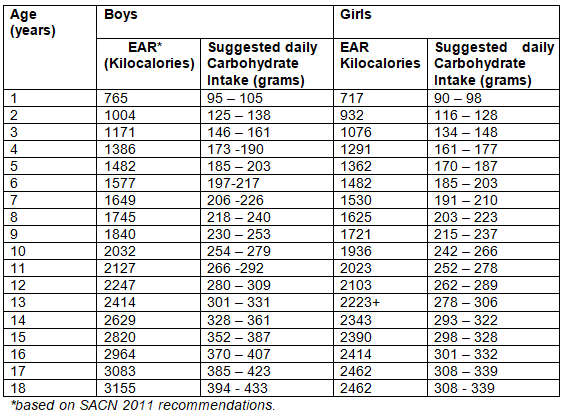
These energy requirements are based on the assumption that the child has normal body composition and takes the recommended amount of exercise. In practice >75% of obese young people are not taking appropriate levels of exercise and so these energy recommendations often need to be reduced by 25%. If healthy eating and portion control have failed then some obese children need to be recommended a much more prescriptive diet i.e. calorie controlled, carbohydrate controlled, increased protein and high fibre according to their individual energy expenditure.
Exercise
Current recommendations advise all children and young people between 5 and 18yrs old should have a minimum of 60 minutes of moderate to vigorous physical activity per day (3 metabolic equivalents) (11). 10000 steps per day is the recommended minimum and equate to around 80 minutes of walking. Strengthening exercises using weights, resistance, or lifting their own body weight, are also recommended for 3 sessions per week for instance gymnastics, climbing, rugby, football., tennis etc. 75% of children are not achieving these minimum levels.
60 minutes of moderate to vigorous physical activity in childhood is associated with improvements in adiposity, cardiovascular risk factors, metabolic syndrome, aerobic fitness, asthma, blood pressure, mental health and academic performance.
Resistance/weights based activities are also recommended now for children > 10 years and are also very effective in improving metabolic health. Going to the gym 3 times weekly has the same effect as 1g twice daily of metformin in the insulin resistant adolescent, and both together are synergistic. Weights used should be light enough to be able to do 12 or more repetitions so as not to damage growth plates.
In addition to encouraging activity, screen time should also be reduced to 2 hours per day. This does not include school work but includes computer based recreational screen time, TV, iPhones etc. It is also helpful to limit long journeys and other long periods of inactivity where possible.
Eating behaviour
Families should be encouraged to sit down together and have regular mealtimes in order to encourage a safe and enjoyable eating environment (12). Children should be encouraged to eat slowly and mindfully, as this results in improved satiety signals and eating less. Children do not need to eat until they are full but only until they are no longer hungry as most obese children have reduced satiety. Stimulus control means avoiding known triggers for overeating such as buffets, uncontrolled portioning and eating in front of the television. If the child is always hungry after school then the main meal should be provided then, or a pre-prepared low calorie filling snack e.g. soup, should be provided so that they can wait for dinner without over consuming.
Self monitoring is extremely important i.e. recording what you are eating so that you can set a limit every day e.g. using ‘my fitness pal’ or a similar app. Children should be weighed 2 weekly if possible as part of self monitoring. It is helpful to set SMART goals at the end of each consultation to clarify and structure eating behaviour. These should be specific, measurable, achievable, realistic and time-based. Rewards should be set for achieving goals. This usually works best if it is a weekly reward associated with quality time with a parent e.g. watching a movie together of going swimming. Financial rewards do not work well. Children are motivated by effort and achievement and so the reward should not be excessive or given too easily. Children should be praised for success to bolster self esteem. The whole family should be following a similar diet as usually they are all obese and parental role modelling improves the chance of success.
Psychological barriers
Significant psychosocial barriers to success should be addressed in a supportive way whenever possible e.g. helping a parents with behavioural support and obtaining psychological or CAMHS management for anxiety and depression.
However persistent denial, lack of engagement and WNBs can require escalation to MASH or children’s services depending on the age of the child and the level of harm being suffered in terms of the child’s co-morbidities and overall functioning.
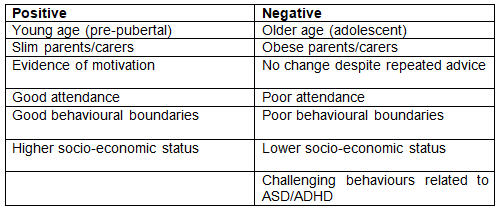
Summary of positive and negative predictors of success
Exercise
Current recommendations advise all children and young people between 5 and 18yrs old should have a minimum of 60 minutes of moderate to vigorous physical activity per day (3 metabolic equivalents) (11). 10000 steps per day is the recommended minimum and equate to around 80 minutes of walking. Strengthening exercises using weights, resistance, or lifting their own body weight, are also recommended for 3 sessions per week for instance gymnastics, climbing, rugby, football., tennis etc. 75% of children are not achieving these minimum levels.
60 minutes of moderate to vigorous physical activity in childhood is associated with improvements in adiposity, cardiovascular risk factors, metabolic syndrome, aerobic fitness, asthma, blood pressure, mental health and academic performance.
Resistance/weights based activities are also recommended now for children > 10 years and are also very effective in improving metabolic health. Going to the gym 3 times weekly has the same effect as 1g twice daily of metformin in the insulin resistant adolescent, and both together are synergistic. Weights used should be light enough to be able to do 12 or more repetitions so as not to damage growth plates.
In addition to encouraging activity, screen time should also be reduced to 2 hours per day. This does not include school work but includes computer based recreational screen time, TV, iPhones etc. It is also helpful to limit long journeys and other long periods of inactivity where possible.
Eating behaviour
Families should be encouraged to sit down together and have regular mealtimes in order to encourage a safe and enjoyable eating environment (12). Children should be encouraged to eat slowly and mindfully, as this results in improved satiety signals and eating less. Children do not need to eat until they are full but only until they are no longer hungry as most obese children have reduced satiety. Stimulus control means avoiding known triggers for overeating such as buffets, uncontrolled portioning and eating in front of the television. If the child is always hungry after school then the main meal should be provided then, or a pre-prepared low calorie filling snack e.g. soup, should be provided so that they can wait for dinner without over consuming.
Self monitoring is extremely important i.e. recording what you are eating so that you can set a limit every day e.g. using ‘my fitness pal’ or a similar app. Children should be weighed 2 weekly if possible as part of self monitoring. It is helpful to set SMART goals at the end of each consultation to clarify and structure eating behaviour. These should be specific, measurable, achievable, realistic and time-based. Rewards should be set for achieving goals. This usually works best if it is a weekly reward associated with quality time with a parent e.g. watching a movie together of going swimming. Financial rewards do not work well. Children are motivated by effort and achievement and so the reward should not be excessive or given too easily. Children should be praised for success to bolster self esteem. The whole family should be following a similar diet as usually they are all obese and parental role modelling improves the chance of success.
Psychological barriers
Significant psychosocial barriers to success should be addressed in a supportive way whenever possible e.g. helping a parents with behavioural support and obtaining psychological or CAMHS management for anxiety and depression.
However persistent denial, lack of engagement and WNBs can require escalation to MASH or children’s services depending on the age of the child and the level of harm being suffered in terms of the child’s co-morbidities and overall functioning.
Summary of positive and negative predictors of success
Medication
Medication can be helpful for selected cases after thorough evaluation. Metformin may be useful in the context of PCOS, metabolic syndrome, insulin resistance or T2DM. CNS stimulants e.g. modafenil may be useful in the context of hypothalamic disease and narcolepsy. Rarely a genetic cause such as leptin deficiency will lead to treatment via Professor S. Farooqi in Cambridge.
Medication can be helpful for selected cases after thorough evaluation. Metformin may be useful in the context of PCOS, metabolic syndrome, insulin resistance or T2DM. CNS stimulants e.g. modafenil may be useful in the context of hypothalamic disease and narcolepsy. Rarely a genetic cause such as leptin deficiency will lead to treatment via Professor S. Farooqi in Cambridge.
Tier 3 MDT and Bariatric Surgery
The tier 3 service continues to develop and in the future we would like to be able to offer a package of MDT inpatient assessment for complex patients via the Bursledon House team. Currently we are unable to obtain funding for bariatric procedures for children in Southampton but we hope to progress this as National Specialist Commissioning continues to develop.
The tier 3 service continues to develop and in the future we would like to be able to offer a package of MDT inpatient assessment for complex patients via the Bursledon House team. Currently we are unable to obtain funding for bariatric procedures for children in Southampton but we hope to progress this as National Specialist Commissioning continues to develop.
Signposting for Self Assessment and further information
www.nhs.uk/change4life/about-change4life
www.nhs.uk/live-well/eat-well/the-eatwell-guide
www.nhs.uk/livewell/healthy-eating/Pages/Healthyeating.aspx
www.nhs.uk/live-well/exercise/physical-activity-guidelines-children-under-five-years/
www.nhs.uk/live-well/eat-well/how-does-sugar-in-our-diet-affect-our-health/
www.infantandtoddlerforum.org/portion-sizes-table-2015
www.bda.uk.com/foodfacts/home
www.nutrition.org.uk/healthyliving
www.mendmoveit.org
www.mendcentral.org
www.nhs.uk/change4life/Pages/change-for-life.aspx
http://www.cwt.org.uk/publications/
www.bupa.co.uk/health-information/p/portion-size
www.nhs.uk/change4life/about-change4life
www.nhs.uk/live-well/eat-well/the-eatwell-guide
www.nhs.uk/livewell/healthy-eating/Pages/Healthyeating.aspx
www.nhs.uk/live-well/exercise/physical-activity-guidelines-children-under-five-years/
www.nhs.uk/live-well/eat-well/how-does-sugar-in-our-diet-affect-our-health/
www.infantandtoddlerforum.org/portion-sizes-table-2015
www.bda.uk.com/foodfacts/home
www.nutrition.org.uk/healthyliving
www.mendmoveit.org
www.mendcentral.org
www.nhs.uk/change4life/Pages/change-for-life.aspx
http://www.cwt.org.uk/publications/
www.bupa.co.uk/health-information/p/portion-size
Assessment proforma for Tier 2
Important points in medical history for those with BMI SDS >2.5
Examination for obesity
Investigations
Important points in medical history for those with BMI SDS >2.5
- Birth weight and gestation and percentile
- Post-natal growth – height in relation to mid-parental height
- Age of onset of obesity
- History of hyperphagia
- Excessive feeing in infancy
- Waking at night demanding food/go looking for food
- Demanding more food immediately after a meal
- Eating rapidly and is not easily distracted from food
- Never feels full
- Has eaten until vomited
- Will consume unpalatable things such as frozen or raw vegetables
- Development
- Hearing
- Vision
- Behaviour
- Gross motor
- Fine motor
- Self care
- Pubertal development
- Early
- Late
- Adrenarche
- Family history
- Consanguinity
- Early-onset obesity
- Diabetes, renal or cardiovascular disease
- Hyperphagia
- Ethnicity
- Co-morbidity
- Diabetes and metabolic syndrome
- NAFLD
- PCOS
- Cardiovascular disease
- Obstructive sleep apnoea
- Psychological problems
- Orthopaedic problems
- Social and educational exclusion
- Gallstones
- Cancers
- Worsening of other conditions e.g. renal disease, asthma
- Other – e.g. reduced physical fitness or mobility
- Dietary history – advise diary or app for 2 weeks
- Exercise history – advise Fitbit or pacer app for 2 weeks
- Impression of motivation – ask the following questions
- What are your concerns?
- What do you think would improve if you could lose weight?
- What have you tried already?
Examination for obesity
- Height, weight, BMI SDS, waist circumference
- Pubertal stage (can be reported rather than formally examined and not always necessary)
- Blood pressure
- Acanthosis nigricans
- Hair colour
- Dysmorphic features
- Pattern of fat distribution: central versus. peripheral
- Striae
Investigations
- Fasted glucose, insulin, C-peptide, HbA1c, LFTs, CRP, lipid profile, TFTs
- Consider OGTT if pubertal with acanthosis nigricans or high risk family history or known fasted insulin resistance
Tier 3 and Bursledon House Pathway
Bursledon House (BH) is a Monday to Friday unit- children go home at weekends. Parents are non resident (visiting 4 – 8 pm with 1 hour pause for children’s evening meal) UNLESS child is preschool/early in reception year in which case parent is resident. Primary school aged children are not permitted to have mobile phones on the unit, and access to ‘devices’ is restricted to after school – all devices are collected at bedtime. BH has a full-time school which liaises closely with home school, so admission does not generally interrupt access to education. We are not registered for post-16 education, hence the upper age restriction.
Criteria for consideration of BH MDT inpatient assessment
Pathway
Bursledon House (BH) is a Monday to Friday unit- children go home at weekends. Parents are non resident (visiting 4 – 8 pm with 1 hour pause for children’s evening meal) UNLESS child is preschool/early in reception year in which case parent is resident. Primary school aged children are not permitted to have mobile phones on the unit, and access to ‘devices’ is restricted to after school – all devices are collected at bedtime. BH has a full-time school which liaises closely with home school, so admission does not generally interrupt access to education. We are not registered for post-16 education, hence the upper age restriction.
Criteria for consideration of BH MDT inpatient assessment
- Able to use the stairs
- Not completed year 11 (GCSE year) at school – in fact, the younger they are the better the likelihood of success.
- Careful consideration needed around oxygen dependency (we have no piped oxygen, cylinders can be organized for established low flow O2 by discussion)
- Child and family have agreed to the admission ‘rules’ above
Pathway
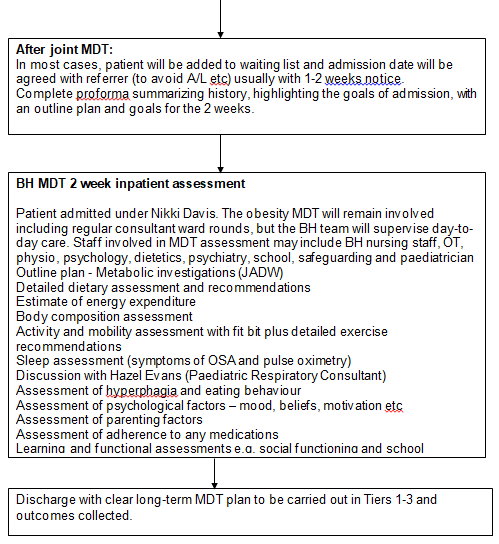
Possible barriers to admission:
Likely goals include:
Outcomes should be collected and included in service evaluation of the obesity tier 3 service. This will be very helpful for commissioners and national specialist commissioning in the future.
- Refusal to sign up to parental non-residence and restricted access to devices. This may require some work with referring team to educate regarding outcomes and long term reward of admission.
- Separation anxiety in child and/or parent. Good integration between the obesity MDT and BH, and introduction of BH early in the tier 3 pathway, may minimize this.
Likely goals include:
- Successful weight management – diet, exercise, medication
- Clear safeguarding boundaries and plan
- Clear plan regarding parenting ability and expectations after discharge
- Improved school functioning
- Clear assessment of balance between organic and environmental factors
- Assessment and preparation for bariatric procedures in the future
- Avoiding expensive and inappropriate hospital admissions
Outcomes should be collected and included in service evaluation of the obesity tier 3 service. This will be very helpful for commissioners and national specialist commissioning in the future.
Appendix B: Genetics of Obesity Assessment Form
(To download, hover over document and click printer icon)
(To download, hover over document and click printer icon)
Appendix C: Bursledon House Pre-Admission Assessment Proforma
(To download, hover over document and click printer icon)
(To download, hover over document and click printer icon)
References
- Childhood obesity: a plan for action - Cabinet Office, Department of Health & Social Care, HM Treasury, Prime Minister’s Office 10 Downingstreet. - GOV.UK. Gov.Uk. 2017. Available at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/546588/Childhood_obesity_2016__2__acc.pdf (last accessed March 2020)
- Public Health England. Health matters: obesity and the food environment. Health Matters. 2017.
- Health and Social Care Information Centre. Statistics on Obesity, Physical Activity and Diet: England, 2017. NHS Digital. 2017.
- Coles N, Birken C, Hamilton J. Emerging treatments for severe obesity in children and adolescents. BMJ. 2016;
- Grover SA, Kaouache M, Rempel P, Joseph L, Dawes M, Lau DCW, et al. Years of life lost and healthy life-years lost from diabetes and cardiovascular disease in overweight and obese people: A modelling study. Lancet Diabetes Endocrinol. 2015;
- Peeters A, Barendregt JJ, Willekens F, Mackenbach JP, Al Mamun A, Bonneux L, et al. Obesity in adulthood and its consequences for life expectancy: A life-table analysis. Ann Intern Med. 2003;
- Warschburger P, Kröller K. Childhood overweight and obesity: Maternal perceptions of the time for engaging in child weight management. BMC Public Health. 2012;
- Tedstone A, Anderson S, Allen R, Targett V, Allen R. Sugar Reduction: The evidence for action. Public Heal Engl. 2015;
- Sears B, Perry M. The role of fatty acids in insulin resistance. Lipids in Health and Disease. 2015.
- Perry B, Wang Y. Appetite regulation and weight control: the role of gut hormones. Nutr Diabetes. 2012;
- Department of Health. Physical activity guidelines for children and young people. Obes Heal Living. 2011;
- Birch L, Arbor A, Savage JS, Ventura A. Influences on the Development of Children’s Eating Behaviours: From Infancy to Adolescence. Can J Diet Pr Res. 2009;
|
Document Version:
1.0 Lead Author: Dr Nikki Davis, Paediatric Consultant Endocrinology & Diabetes Additional Author: James Barrett, Paediatric Dietician |
Approving Network:
Paediatric Nutrition and Hydration Group Date of Approval: 03/2020 Review Date: 03/2023 |
PIER Contact |
|