Bedside Placement and Care of a Nasojejunal Tube
Flowchart
Introduction
The aim of this document is to provide a short summary guideline for the bedside placement of a Nasojejunal tube (NJ tube). A routine nasogastric tube (NG tube) is not needed but in special circumstances both an NG tube and an NJ tube maybe required.
Scope and Purpose
This guideline is for use by all Registered Nursing staff (band 4 and up) and medical staff that provide care for children with differing physical, psychological, social and emotional needs who require a NJ tube. The aim of this guideline is guide staff in the placement of an NJ tube on the ward. It outlines the clinical standards required for safe and competent care when placing and feeding a child via an NJ tube
Scope and Purpose
This guideline is for use by all Registered Nursing staff (band 4 and up) and medical staff that provide care for children with differing physical, psychological, social and emotional needs who require a NJ tube. The aim of this guideline is guide staff in the placement of an NJ tube on the ward. It outlines the clinical standards required for safe and competent care when placing and feeding a child via an NJ tube
Definitions
Nasogastric Tube (NG tube)
A narrow bore tube passed into the stomach via the nose. It is used for short / medium / long term nutritional support; also for aspiration of stomach contents – e.g. for decompression of intestinal obstruction
Naso/oro jejunal tube (NJ tube)
A narrow bore long term tube passed into the small bowel (jejunum) via the nose. It is used for short / medium / long term nutritional support. For the purposes of this guideline naso/ oro jejunal tubes will be referred to as NJ tube, although it is recognised in some circumstances an orogastric tube will be required.
NEX measurement
Nose; Ear; Xiphisternum measurement – this is how to measure the length of an NG tube.
pH indicator strip
An indicator strip that shows level of acidity
Gastric decompression
The removal of pressure caused by gas or fluid from the stomach.
Turbulent Flush
Using a push stop, push stop technique on the syringe rather than a slow steady push
A narrow bore tube passed into the stomach via the nose. It is used for short / medium / long term nutritional support; also for aspiration of stomach contents – e.g. for decompression of intestinal obstruction
Naso/oro jejunal tube (NJ tube)
A narrow bore long term tube passed into the small bowel (jejunum) via the nose. It is used for short / medium / long term nutritional support. For the purposes of this guideline naso/ oro jejunal tubes will be referred to as NJ tube, although it is recognised in some circumstances an orogastric tube will be required.
NEX measurement
Nose; Ear; Xiphisternum measurement – this is how to measure the length of an NG tube.
pH indicator strip
An indicator strip that shows level of acidity
Gastric decompression
The removal of pressure caused by gas or fluid from the stomach.
Turbulent Flush
Using a push stop, push stop technique on the syringe rather than a slow steady push
Bedside Placement of a Nasojejunal Tube
Please see flow diagram at beginning of document
Placement of a feeding tube into the small bowel
The decision to place the tube in the duodenum (the first section of the small bowel) or the jejunum (the second section of the small bowel) depends on the clinical condition of the child. It must be document in the child’s health records.
Jejunal feeding may be initiated in any age group of patients following discussion with the wider multi-disciplinary team.
Considerations for jejunal feeding are:
Contraindications for jejunal feeding are:
Consideration for orojejunal rather than naso-jejunal tube:
• Basal skull fracture
• Maxillo facial abnormalities
• Nasopharyngeal abnormalities
Please consider the following points before initiating jejunal feeding
If you are considering a referral to the paediatric gastroenterology team; please discuss the placement of an NJ tube with the gastroenterology team first.
Consideration and documentation of the following is imperative before placing an NJ tube:
Indication for placing an NJ tube?
Recurrent replacement of an NJ tube is an invasive procedure
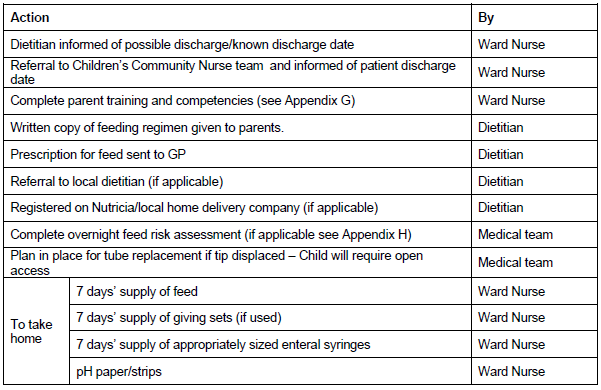
Considerations for Patient Discharge
Placement of a feeding tube into the small bowel
The decision to place the tube in the duodenum (the first section of the small bowel) or the jejunum (the second section of the small bowel) depends on the clinical condition of the child. It must be document in the child’s health records.
Jejunal feeding may be initiated in any age group of patients following discussion with the wider multi-disciplinary team.
Considerations for jejunal feeding are:
- Severe gastro oesophageal reflux
- Delayed gastric emptying
- Persistent vomiting
- Trauma e.g. traumatic brain injury (TBI)
- Malignancy
Contraindications for jejunal feeding are:
- Bowel obstruction
- Oesophageal atresia/stenosis
- Significant upper GI bleeding
- Necrotising enterocolitis (conservative management)
- Ischaemic bowel
Consideration for orojejunal rather than naso-jejunal tube:
• Basal skull fracture
• Maxillo facial abnormalities
• Nasopharyngeal abnormalities
Please consider the following points before initiating jejunal feeding
If you are considering a referral to the paediatric gastroenterology team; please discuss the placement of an NJ tube with the gastroenterology team first.
Consideration and documentation of the following is imperative before placing an NJ tube:
Indication for placing an NJ tube?
- Growth (height and weight)
- Continuous gastric feeding with breaks should be tried. A regimen of 10 hours of continuous feeding followed by a 2 hours break and repeat.
- Fully understand the risks and benefits associated with NJ tubes; including the risk of recurrent displacement.
- Full and frank discussion with multi-disciplinary team
- Plan for tube replacement post discharge
- Patient follow-up and exit strategy
Recurrent replacement of an NJ tube is an invasive procedure
- Displacement is more likely in:
- younger children
- children with neurological movement disorders
- those with recurring vomiting (particularly retching) as they will vomit out the tube
- NJ tubes can be placed on ward following this guideline
- If NJ placement is unsuccessful on the ward (following 2 attempts) discussion with radiology is required for fluoroscopic placement.
Considerations for Patient Discharge
Appendix B - Equipment Required for Jenjunal Tube Placement
- Naso-jejunal tube (6 – 8 Fr long term tube with a guidewire) – Consider the child’s age, nasal cavity size and other relevant anatomical considerations when deciding on size of tube
- Plastic apron and gloves – mouth and eye protection should be available
- Hand gel
- Tape (or nasal tube fixation device)
- Tape measure
- Syringe
- Water for lubrication
- Sterile water in hospital
- pH indicator strip (check expiry date)
- Vomit bowl and Tissues
- Oxygen and suction (check both are working)
- Prepared medication or feed
- A drink with a straw or a dummy for a child to suck on (if appropriate)
- Drainage bag if to have an NG on drainage as well
Appendix C - Aspiration of a Nasojejunal Tube
This should only be attempted by those trained to do so if there are concerns that the NJ tube has displaced based on clinical judgement.
- Gently push 5ml of air into the tube, briefly remove the syringe, reattach and then attempt to draw back. If a vacuum is present, this is an indicator that the tip of the tube is within the intestine.
- If air can be drawn back up the tube, this is a strong indicator that the end of the tube is in the stomach.
- The smallest size syringe that must be used to aspirate the tube is a 10ml.
- A vacuum should be felt when aspirating an NJ tube, this is normal for a Jejunal aspirate.
- Fluids pass through the jejunum and do not accumulate within it, as in the stomach, obtaining an aspirate can be a timely process and may not be possible, thus if the other indicators are acceptable, an aspirate is not required.
- Pulling against a vacuum is the only way to achieve an aspirate from the jejunum, but excessive pressure on the tube can contribute to its displacement from the intestine.
- If an aspirate is obtained, test pH (if below 5 most likely gastric content)
- A record must be maintained showing the length of the NJ tube at the nostril, as from initial placement, which was confirmed by screening fluoroscopy or x-ray. This must be recorded daily whilst in hospital.
- Of Note
- Prior to feed/medication/water being administered, the length of the tube should be checked and documented (see appendix F).
- As the numbers wear off the NJ tube once it has been in place for a while, the tube should be marked with a black line at the nostril, to indicate correct placement length.
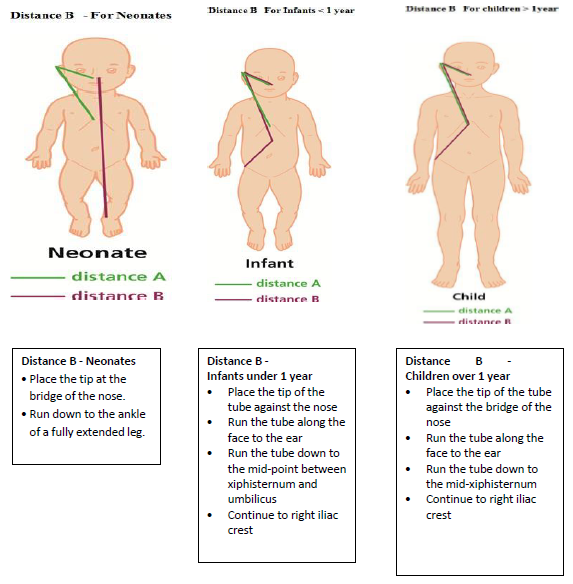
Appendix D - Measuring for a Nasojejunal Tube
It important to determine the length of NJ TUBE required to reach the jejunum prior to insertion. This should be done in two measurements A and B:
Distance B (is measured according to age)
- Distance A: This is the NEX measurement (nose, ear, xiphisternum) as per a nasogastric tube
- Distance B: The length of tube required to place an NJ tube in the small bowel. See pictures below for the different age groups. Oral jejunal tubes should be measured from the mouth and not the nose for all age groups. The measurements are obtained as follows:
Distance B (is measured according to age)
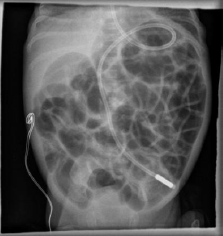
Appendix E - X-Ray Interpretation
The NJ tube tip should been seen to go through the pylorus and around the c-shaped duodenum. The tip should ideally lie either in the midline (over a vertebral body) or to the left of the patients midline in the jejunum (picture 1).
- If NJ tube is too far in e.g. seen to curl in small bowel loops gently withdraw as necessary. You can measure the exact distance to withdraw on the X-ray.
- If NJ tube is through the pylorus but lies short, then loosen the securing tapes and advance further as necessary. Re-X-ray to confirm final position before feeding is commenced.
- If there is any uncertainty about the position of an NJ tube, please discuss with a radiologist before the tube is removed.
- If NJ tube is coiled in the stomach, without going through the pylorus discuss with radiology before attempting a second placement.
- If the NJ tube has taken an unusual path within the bowel discuss with the radiologist before removal of the tube (picture 2).
|
Picture 1 - Correct Placement

|
Picture 2
|
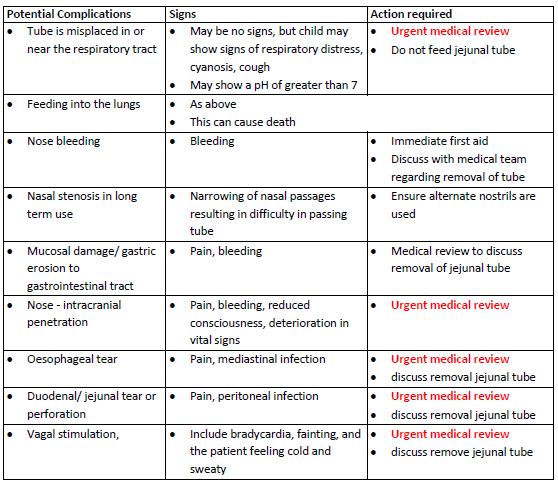
Appendix F - Potential Complications of Jejunal Tube Placement
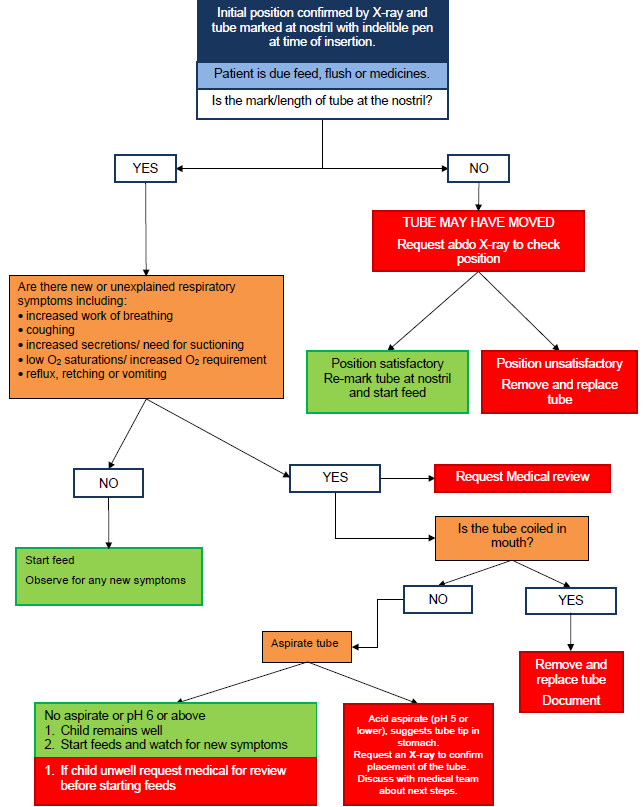
Appendix G - Nasojejunal Tube Position Check Pathway (Inpatient)
Document All Decisions and Actions
Document All Decisions and Actions
Appendix H - Nasojejunal Tube Teaching for Parents and Carers
References
- Adams D (1994) Administration of drugs through a jejunostomy tube. British Journal of Intensive Care Jan: 10-17
- Auckland District Health Board (2014) Newborn Services Clinical Guideline. ADHB, New Zealand. [Accessed 9 July 2014]
- Courtney-Moore M (1985) Tube feeding of infants and children. Paediatric Clinics of North America 32(2): pp 401-405
- De lucas, C (2000). Transpyloric enteral nutrition reduces the complication rate and cost in critically ill child, Journal of Pediatric gastroenterology and nutrition 30(2): 175-180
- Johnson T (2014) Enteral Nutrition. In: Shaw V (ed) Clinical Paediatric Dietetics, 4th Edition. Oxford, Wiley Blackwell
- Knox, T and Davie, J (2009) Nasogastric tube feeding-which syringe size produces lower pressure and is safest to use? Nursing Times 105(27): 24-26
- Mayer R, Harrison S, Cooper M, Habibi P. Successful blind placement of naso-jejunal tubes in paediatric intensive care: impact of training and audit. JAN: 2007: 402 - 408
- Muscari-Lin E (1991). Nutrition support: making the difficult decisions. Cancer Nursing 14(5): 261-269
- National Patient Safety Agency (NPSA) (2011). Reducing the harm caused by misplaced nasogastric feeding tubes in adults, children and infants. Patient Safety Alert NPSA/2011/PSA002, London. [Accessed 11 November 2014]
- National Patient Safety Agency (NPSA) (2005) Reducing the harm caused by misplaced naso and orogastric feeding tubes in babies under the care of neonatal units. Patient Safety Alert NPSA/2005/9, London. [Accessed 11 November 2014]
- Royal College of Nursing (2010) Restrictive physical intervention and therapeutic holding for children and young people. London. [Accessed 11 November 2014]
- McDermott A , Tomkins N , Lazonby G (2007) Naso-jejunal tube placement in paediatric intensive care. Paediatric Nursing 19(2): 26-28
- Ashford and St Peters Hospitals (2012) Neonatal Intensive Care Unit Clinical Guideline – Naso-jejunal (NJT) insertion
- Rees RGP, Payne-James JJ, King C et al. (1998) Spontaneous transpyloric passage and performance of fine bore polyurethane feeding tubes. A controlled clinical trial. J Parent Ent Nutr, 12: 469–472
- Mason S, Harris G, Blisset J (2005) Tube feeding in infancy: implications for the development of normal eating and drinking skills. Dysphagia, 20:46−61
- Shaw V (2015) Clinical Paediatric Dietetics, 4th Edition. Oxford, Wiley Blackwell
- Everitt L, Dick K, Pridgeon J, et al (2016) G30 Paediatric Jejunal feeding is resource intensive; report of 5 year practice in Wessex Archives of Disease in Childhood 101:A21- A22. (http://dx.doi.org/10.1136/archdischild-2016-310863.29)
|
Document Version:
2.0 Lead Authors: Karen Dick & Maddie Allam (Paediatric Surgical Specialist Nurses) |
Approving Network:
Wessex Paediatric Gastroenterology Network Date of Approval: September 2021 Review Due:
September 2024 |
PIER Contact |
|