Paediatric Viral Induced Wheeze and Acute Asthma Treatment Pathway
Introduction
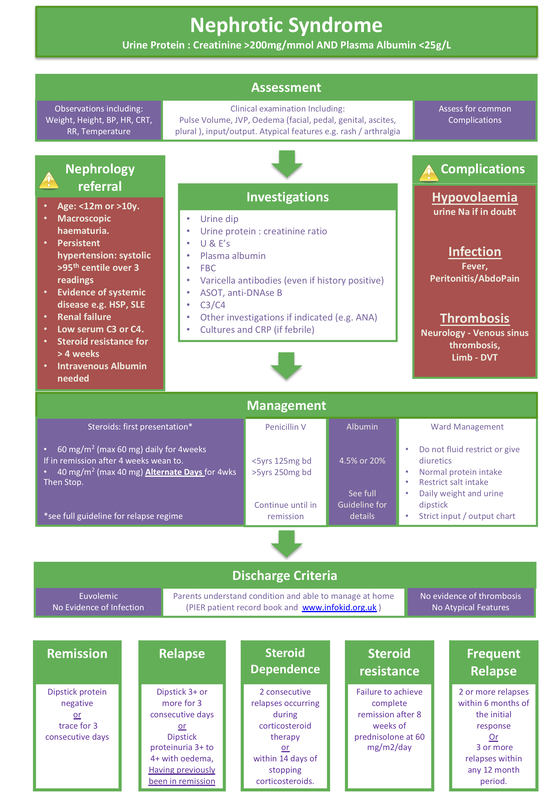
Nephrotic syndrome refers to any condition in which there is heavy proteinuria and hypoalbuminemia. A urine protein:creatinine ratio of >200mg/mmol and a plasma albumin of <25g/L are the diagnostic parameters required for a diagnosis.
In children, steroid sensitive Nephrotic Syndrome can be broadly divided into 3 groups:
Minimal change disease (MCD) also known as steroid sensitive disease. This accounts for 78% of cases. The peak age of onset of minimal change (steroid sensitive) nephrotic syndrome is 2½ years; 80% have presented by 6 years of age. Other types of Nephrotic Syndrome tend to present in older children. Focal segmental glomerulosclerosis (FSGS) accounts for 8% of cases and Membranoproliferative glomerulonephritis (MPGN) for 6%.
The annual incidence of nephrotic syndrome is approximately 2/100,000 children under 16 years of age. It is more common in Asians (about 7/100,000/year). The cumulative prevalence is about 16/100,000.
Nephrotic syndrome refers to any condition in which there is heavy proteinuria and hypoalbuminemia. A urine protein:creatinine ratio of >200mg/mmol and a plasma albumin of <25g/L are the diagnostic parameters required for a diagnosis.
In children, steroid sensitive Nephrotic Syndrome can be broadly divided into 3 groups:
Minimal change disease (MCD) also known as steroid sensitive disease. This accounts for 78% of cases. The peak age of onset of minimal change (steroid sensitive) nephrotic syndrome is 2½ years; 80% have presented by 6 years of age. Other types of Nephrotic Syndrome tend to present in older children. Focal segmental glomerulosclerosis (FSGS) accounts for 8% of cases and Membranoproliferative glomerulonephritis (MPGN) for 6%.
The annual incidence of nephrotic syndrome is approximately 2/100,000 children under 16 years of age. It is more common in Asians (about 7/100,000/year). The cumulative prevalence is about 16/100,000.
Presentation
Oedema is the usual presenting feature, classically with periorbital eye oedema, more pronounced in the morning. Pedal, ankle and genital oedema are also common, the latter may be painful. Other symptoms include; lethargy, shortness of breath, chest pain, frothy urine, diarrhoea, vomiting, poor appetite.
Oedema is the usual presenting feature, classically with periorbital eye oedema, more pronounced in the morning. Pedal, ankle and genital oedema are also common, the latter may be painful. Other symptoms include; lethargy, shortness of breath, chest pain, frothy urine, diarrhoea, vomiting, poor appetite.
Complications
- Hypovolaemia. Typically occurs early in a relapse. May be precipitated by diarrhoea, sepsis and inappropriate diuretic therapy. Drainage of ascites or pleural effusions can also precipitate hypovolaemia.
- Infection. Especially with encapsulated organisms such as Strep. pneumoniae or H. influenzae type b. Steroid and other immunosuppressive therapy increases the risk of viral infections e.g. varicella.
- Thrombosis. Due to an acquired hyper-coagulable state and haemoconcentration. May be venous, or less commonly arterial
Prognosis (steroid sensitive)
- 30% have no relapses or only 1 relapse.
- 40% have infrequent relapses.
- 30% have frequent relapses or are steroid dependant.
- Mortality is 1-3%, mostly from infection or thrombosis.
- About 90% enter permanent remission by, or during adolescence.
- Minimal change nephrotic syndrome does not usually progress to chronic renal failure, but may be complicated by acute renal failure during episodes of hypovolaemia and/or infection.
- Some patients are initially steroid sensitive and develop secondary steroid resistance. Secondary steroid resistance is an indication for referral to a nephrologist and indicates a poorer prognosis
Classifications
Nephrotic syndrome: Early morning urine protein: creatinine ratio > 200 mg/mmol and plasma albumin < 25 g/l.
Remission: Dipstick protein negative or trace for 3 consecutive days.
Relapse (having previously been in remission):
Dipstick 3+ or more for 3 consecutive days or Dipstick proteinuria 3+ to 4+ with oedema.
Frequent relapses: 2 or more relapses within 6 months of the initial response or 3 or more relapses within any 12 month period.
Steroid dependence: 2 consecutive relapses occurring during corticosteroid therapy or within 14 days of stopping corticosteroids.
Steroid resistance: Failure to achieve complete remission after 8 weeks of prednisolone at 60 mg/m2/day.
Nephrotic syndrome: Early morning urine protein: creatinine ratio > 200 mg/mmol and plasma albumin < 25 g/l.
Remission: Dipstick protein negative or trace for 3 consecutive days.
Relapse (having previously been in remission):
Dipstick 3+ or more for 3 consecutive days or Dipstick proteinuria 3+ to 4+ with oedema.
Frequent relapses: 2 or more relapses within 6 months of the initial response or 3 or more relapses within any 12 month period.
Steroid dependence: 2 consecutive relapses occurring during corticosteroid therapy or within 14 days of stopping corticosteroids.
Steroid resistance: Failure to achieve complete remission after 8 weeks of prednisolone at 60 mg/m2/day.
Scope
This guideline applies to all paediatric patients in the region but not to neonates on neonatal units.
This guideline applies to all paediatric patients in the region but not to neonates on neonatal units.
Purpose
The purpose of this guideline is to describe to provide a standardised approach to the management of Childhood Nephrotic Syndrome.
The purpose of this guideline is to describe to provide a standardised approach to the management of Childhood Nephrotic Syndrome.
Management
Management of the Initial Episode
Confirm diagnosis
Perform the following observations:
History and Examination.
Ensure you assess for the common complications.
Investigations
Inpatient Management of Nephrotic Syndrome
Admit to confirm diagnosis, manage complications, educate parents and commence therapy. If the patient is stable it is not necessary to keep the patient in hospital until remission is achieved.
Indications for admission
Ward Management
Indication for referral to a Nephrologist
*A useful way to estimate renal function is to use the modified Schwartz formula:
GFR (ml/min/1.73m2) = height in cm x 40/plasma creatinine in μmol/l. Normal range is 80-130 for children over 18 months.
** Steroid resistance is from 8 weeks, the nephrology team want to know at 4 weeks.
Management of the Initial Episode
Confirm diagnosis
- Urine protein : creatinine ratio >200mg/mmol and plasma albumin <25g/L.
Perform the following observations:
- Weight, height, BP (calculate BP centiles), HR, capillary refill time (CRT), RR, temperature.
History and Examination.
- Ensure your clinical examination includes assessment of fluid status. Look for signs of intravascular depletion and extra vascular fluid (oedema). This should include peripheral perfusion, pulse volume, JVP, history of input/output. Look for oedema around the face, feet and genitals, assess for pleural effusion and ascites. Ensure you ask about atypical features such as joint pains and assess for rashes.
Ensure you assess for the common complications.
- Infection: remember unusual infections such as peritonitis.
- Thrombosis: neurological signs such as seizures could indicate a venous sinus thrombosis. Limb pain and swelling could indicate a DVT.
- Hypovolaemia: assess as above.
Investigations
- Urine Dip (Early morning urine, EMU)
- Urine protein:creatinine ratio (EMU)
- Sodium, potassium, urea, creatinine
- Plasma albumin
- FBC
- Varicella antibodies (even if history positive)
- ASOT, anti-DNAse B
- C3/C4
- Other investigations if indicated (e.g.ANA)
- Cultures and CRP (if febrile)
Inpatient Management of Nephrotic Syndrome
Admit to confirm diagnosis, manage complications, educate parents and commence therapy. If the patient is stable it is not necessary to keep the patient in hospital until remission is achieved.
Indications for admission
- Parent education
- Age < 12 months or > 10 years
- Macroscopic haematuria
- Persistent hypertension
- Evidence of systemic disease e.g. HSP, SLE
- Renal failure
- Intravenous albumin required
- Poor perfusion
- Severe oedema / ascites / pleural effusions
- Severe intercurrent infection
Ward Management
- Daily weights.
- Daily urine dipstick.
- Regular observations (obs) with blood pressures.
- Strict fluid balance. Measure all drinks and all urine output.
- Normal protein intake (increase if malnourished).
- Restrict salt intake: “no added salt” diet while in relapse or on high dose steroids.
- Avoid arterial stabs except in critical situations because of risk of arterial thrombosis.
- Initiate medical therapy.
- Liaise with Nephrology team as appropriate.
- Do not fluid restrict or give diuretics. Patients with “pure” nephrotic syndrome (i.e. no features
of nephritic syndrome, sustained hypertension, renal failure or macroscopic haematuria) are typically intravascularly depleted during relapse. Fluid restriction and aggressive diuretic therapy are therefore inappropriate.
Indication for referral to a Nephrologist
- Macroscopic haematuria
- Persistent hypertension
- Steroid resistance (from 4 weeks onwards)**
- Low serum C3 or C4
- Intravenous albumin indicated.
- Evidence of systemic disease e.g. HSP, SLE.
- Age < 12 months or > 10 years
- Renal failure* (excludes minor reversible pre-renal element common with steroid sensitive nephrotic syndrome)
*A useful way to estimate renal function is to use the modified Schwartz formula:
GFR (ml/min/1.73m2) = height in cm x 40/plasma creatinine in μmol/l. Normal range is 80-130 for children over 18 months.
** Steroid resistance is from 8 weeks, the nephrology team want to know at 4 weeks.
Treatment
Steroids, Steroid sparing drugs, Antibiotics
Steroids (prednisolone) - First presentation
Steroids – Relapse (but not FREQUENT RELAPSES)
Frequent relapsers and steroid dependent nephrotics
Antibiotics
Albumin: 20% and 4.5%
The use of intravenous 20% albumin should always be discussed with a paediatric nephrologist. Do not give 20% albumin to treat low serum albumin. The indications for 20% albumin are clinical.
Indications:
Risks of 20% albumin: Hypertension & Pulmonary Oedema – can occur several hours post infusion
Infusion of 20% albumin solution can cause 5 times the infused volume of fluid to be drawn into the circulation. This may result in pulmonary oedema and hypertension if infusion is too rapid or the patient has renal impairment. If peripheral perfusion or urine output are poor 4.5% albumin may be safer than using 20% albumin. Once the patient is passing good volumes of urine 20% albumin can be used.
Dosing
Monitoring
Due to the risks of 20% albumin you need commence the infusion in an HDU or high obs bed. Do not give it overnight.
Before you start ensure you have calculated the BP centiles and normal ranges of observation have been agreed with the nursing and medical staff. When giving 20% albumin the strict input / output chart must continue.
Ensure continuous HR and sats monitoring throughout the infusion. A blood pressure, RR and temperature should be done with every set of observations. Observations need to be done at:
Any evidence of circulatory overload (high HR, high BP) or pulmonary oedema (low sats, high RR) stop the infusion and get an urgent medical review.
Steroids, Steroid sparing drugs, Antibiotics
Steroids (prednisolone) - First presentation
- 60mg/m2 (max 60mg) daily for 4 weeks
- If in remission after 4 weeks wean as below – if not in remission discuss with a Nephrologist.
- 40mg/m2 (max 40mg) alternate days for 4wks
- Stop (total of 8weeks)
Steroids – Relapse (but not FREQUENT RELAPSES)
- First relapse
- Admission is often not necessary
- Give prednisolone 60mg/m2/day (max 60mg) until remission.
- Then reduce dose to 40mg/m2 alternate days for 4 weeks, then stop
- Subsequent relapse
- Individualised weaning schedule dependant on previous history
- Most will require a longer wean (up to 12 weeks)
Frequent relapsers and steroid dependent nephrotics
- These require consultation with a nephrologist. The below treatment is to be instigated by tertiary Nephrology and is for your information only. Drugs used include:
- Low dose, alternate day steroids therapy
- Levamisole
- Cyclophosphamide
- Tacrolimus
- Mycophenolate Mofetil (MMF)
- Rituximab
Antibiotics
- Prophylactic Penicillin V, continue until in remission
- <5yrs 125mg bd
- 5yrs 250mg bd
Albumin: 20% and 4.5%
The use of intravenous 20% albumin should always be discussed with a paediatric nephrologist. Do not give 20% albumin to treat low serum albumin. The indications for 20% albumin are clinical.
Indications:
- Severe oedema
- Ascites splinting the diaphragm
- Pleural effusions affecting respiration- marked discomfort
- Marked scrotal or labial swelling
- Poor perfusion
- Severe intercurrent infections
Risks of 20% albumin: Hypertension & Pulmonary Oedema – can occur several hours post infusion
Infusion of 20% albumin solution can cause 5 times the infused volume of fluid to be drawn into the circulation. This may result in pulmonary oedema and hypertension if infusion is too rapid or the patient has renal impairment. If peripheral perfusion or urine output are poor 4.5% albumin may be safer than using 20% albumin. Once the patient is passing good volumes of urine 20% albumin can be used.
Dosing
- 20% albumin 5ml/kg over 4 hours. IV frusemide 1mg/kg halfway through infusion (unless still clinically hypovolaemic)
- 4.5% Albumin 5-10ml/kg IV over 2 hours
Monitoring
Due to the risks of 20% albumin you need commence the infusion in an HDU or high obs bed. Do not give it overnight.
Before you start ensure you have calculated the BP centiles and normal ranges of observation have been agreed with the nursing and medical staff. When giving 20% albumin the strict input / output chart must continue.
Ensure continuous HR and sats monitoring throughout the infusion. A blood pressure, RR and temperature should be done with every set of observations. Observations need to be done at:
- Baseline (before the infusion)
- 15 mins after start of infusion
- Hourly through out the infusion and for 2 hours afterwards
- If remains stable can be 4 hourly from then on
Any evidence of circulatory overload (high HR, high BP) or pulmonary oedema (low sats, high RR) stop the infusion and get an urgent medical review.
Discharge
Discharge Criteria
Discharge Criteria
- Euvolemic.
- No evidence of infection.
- No evidence of thrombosis.
- No atypical features (needs to be discussed with Nephrologist / Senior Paediatrician before
discharge). - Parents understand the condition and are able to manage at home. Parents should have been
talked through the www.infokid.org information on Nephrotic Syndrome. - The Medicine for children leaflet on prednisolone should be given with the dispensed
medication. - Patient Record Booklet - The patient record book can be printed by clicking here.
When printing please ensure you print TWO SIDED with the instruction to FLIP ALONG SHORT EDGE.
Implementation
Local leads for critically ill children will disseminate guideline and raise awareness locally.
Local leads for critically ill children will disseminate guideline and raise awareness locally.
References
- Consensus statement on management and audit potential for steroid responsive nephrotic syndrome. Report of a Workshop by the British Association for Paediatric Nephrology and Research Unit, Royal College of Physicians. Arch Dis Child. 1994 Feb;70(2):151-7.
- Hodson EM, Knight JF, Willis NS, Craig JC Corticosteroid therapy for nephrotic syndrome in children (Cochrane Review).Cochrane Database Syst Rev. 2001;2:CD001533.
- Durkan AM, Hodson EM, Willis NS, Craig JC. Immunosuppressive agents in childhood nephrotic syndrome: a meta-analysis of randomized controlled trials. Kidney Int. 2001 May;59(5):1919-27.
- Hodson EM, Knight JF, Willis NS, Craig JC. Corticosteroid therapy in nephrotic syndrome: a meta-
analysis of randomised controlled trials. Arch Dis Child. 2000 Jul;83(1):45-51. - Donia AF, Amer GM, Ahmed HA, Gazareen SH, Moustafa FE, Shoeib AA, Ismail AM, Khamis S,
Sobh MA. Levamisole: adjunctive therapy in steroid dependent minimal change nephrotic
children. Pediatr Nephrol. 2002 May;17(5):355-8. - Alsaran K, Grisaru S, Stephens D, Arbus G. Levamisole vs. cyclophosphamide for frequently-
relapsing steroid-dependent nephrotic syndrome. Clin Nephrol. 2001 Oct;56(4):289-94. - Haws RM, Baum M. Efficacy of albumin and diuretic therapy in children with nephrotic
syndrome. Pediatrics. 1993 Jun;91(6):1142-6. - Schweda F, Liebl R, Riegger GA, Kramer BK. Tacrolimus treatment for steroid- and cyclosporin-
resistant minimal-change nephrotic syndrome. Nephrol Dial Transplant 1997 Nov;12(11):2433-5. - Chandra M, Susin M, Abitbol C. Remission of relapsing childhood nephrotic syndrome with
mycophenolate mofetil. Pediatr Nephrol 2000 Mar;14(3):224-6. - PREDINOS study and Cochrane review discussed at regional Nephrology meeting and decision to
change to one month weaning regime made.
|
Document Version:
1.0 Lead Author: Dr Shuman Haq, Consultant Nephrologist, UHS Additional Authors: Dr Kate Goyder, Consultant Paediatrician, Poole Hospital Rosemary Dempsey, Pharmacist, UHS Andy Fox, Pharmacist, UHS |
Approving Network:
Renal Network Date of Approval: 11/1/18 Review Date: November 2021 |
PIER Contact |
|