Initial Management of Hyperthyroidism and Thyrotoxicosis
Introduction
Hyperthyroidism is a relatively uncommon disorder in childhood and adolescence with an incidence of 0.94 per 100,000 children less than 15 years of age.
Scope and Purpose
The purpose of this guideline is to support the general paediatrician with the initial assessment and management of a child presenting with hyperthyroidism.
Hyperthyroidism is a relatively uncommon disorder in childhood and adolescence with an incidence of 0.94 per 100,000 children less than 15 years of age.
Scope and Purpose
The purpose of this guideline is to support the general paediatrician with the initial assessment and management of a child presenting with hyperthyroidism.
Definitions
Definitions
Causes of thyrotoxicosis include:
- FBC – Full Blood Count
- LFT – Liver Function Test TFT – Thyroid Function Test FT3 – Free Triiodothyronine (T3)
- FT4 - Free Thyroxine (T4)
- PTU - Propylthiouracil
- TSH – Thyroid Stimulating Hormone
- USS - Ultrasound scan BNFC – British National Formulary for Children
- Hyperthyroidism is a pathological state caused by increased secretion of thyroid hormones (T4 and/ or T3) from the thyroid gland.
- Thyrotoxicosis refers to the clinical picture caused by hyperthyroidism due to thyroid hormone excess.
Causes of thyrotoxicosis include:
- Graves’ disease
- Hashimoto’s disease
- Infectious thyroiditis - viral or bacterial
- Toxic nodule
- Drug-induced e.g. amiodarone, thyroxine
- Activating TSH receptor mutations
Clinical Features of Thyrotoxicosis
Hyperthyroidism can be asymptomatic in approximately 10% of cases (subclinical hyperthyroidism
Key Points in the History
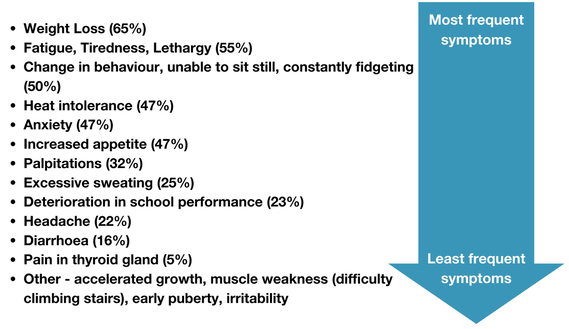
There can be several presenting symptoms and some are more consistent than others. A national survey (BPSU) showed the order of frequency (%) of symptoms as follows:
It is also important to enquire about features and /or history of other autoimmune diseases e.g. diabetes, coeliac disease, Addison’s disease.
Clinical Practice Point
Document whether there is a history of bronchospasm or asthma, as if a beta blocker is required for symptomatic relief, the presence of these features may guide the decision for the choice treatment (see below).
Key Points in the Examination
There may be no clinical features (sub-clinical hyperthyroidism). The following are presenting signs of hyperthyroidism in decreasing order of frequency:

Document height, weight and pubertal status
Investigations
- TSH
- FT4
- FT3*
- CRP
- FBC
- LFT
- Thyroid peroxidase antibodies
- TSH receptor antibodies
- In severe cases consider ECG and echocardiogram
- Request thyroid USS this should be done within 4 weeks of diagnosis
Diagnosis
The following biochemical changes indicate thyrotoxicosis:
- TSH low or undetectable, FT4 high, FT3 high
- TSH low or undetectable, FT4 high, FT3 normal
- TSH low or undetectable, FT4 normal, FT3 high
Clinical Practice Point
If the TSH is not suppressed, alternative diagnoses should be considered.
Treatment
If marginally elevated thyroid hormones and patient asymptomatic, consider not starting treatment and monitoring trend in thyroid function and change in clinical features
1. Carbimazole
- check results of FBC and LFT before starting treatment
- if neutrophils > 1x 109 /L and liver enzymes < 3 x upper limit of normal, start carbimazole as follows (see BNFC):
- < 11 years of age : 0.75 mg/kg/day OD
- > 11 years 30 mg OD
2. Beta Blockers
If there are toxic features consider starting a beta blocker:
- start propranolol oral 250-500 microg/kg 8 hourly (max 40mg per dose, see BNFC antithyroid section). Do not start propranolol if there is a history of bronchospasm or asthma as it is contra-indicated.
- If there is a history of bronchospasm or asthma then atenolol should be used with caution. Suggested starting doses (see BNFC for further information):
- < 12 year 0.5-2mg/kg/day (max 100mg per dose)
- > 12 years 25 – 50 mg daily (max 100mg per dose
Counsel Family/Patient
- Carbimazole is the only and best medical therapy for reducing thyroid hormone levels (by reducing thyroid hormone synthesis):
- Document in the notes that the family have been informed of the rare side effect of agranulocytosis. Inform family/patient to seek medical advice and to get a FBC checked urgently if there is a persistent pyrexia or sore throat
- State other side effects:
- Common – rash, joint pain/swelling
- Rare - headache, GI disturbance, hair loss, agranulocytosis, jaundice, aplastic anaemia, ANCA vasculitis
- Provide written information to family about carbimazole.
- Inform side effects of beta blocker. Propranolol – rare side effects include alopecia, neuromuscular dysfunction, postural hypotension, psychosis and thrombocytopaenia. Inform parents/patient there must be strict medicine adherence – parents to supervise medicine administration if there are concerns for adherence.
- Warn parents/patient once treatment started there is a risk of rapid weight gain as the metabolism has been too fast and will return to normal - advise weight monitoring and calorie restriction if required
- Recommend discontinuing physical exercise until thyroid hormone within normal range
- Inform parents/patient to let school know, as the diagnosis may account for deterioration in school performance, change in behaviour, poor exam results
Discharge Planning
- Organise a repeat TFT and FT3 in 2 weeks
- Refer to ophthalmology as an outpatient if there are thyroid eye signs
- Chase the results of the antibodies and thyroid USS
- During working hours inform the local paediatrician with an interest in endocrinology and arrange a follow-up appointment with them. This can be found through the Endocrine Network.
- Provide the Patient information leaflet. This can be printed off and given to parents or young person here.
Thyroid Storm
A thyroid storm is a very rare and extreme form of thyrotoxicosis. It can be precipitated by incompletely treated thyrotoxicosis, major trauma, stress, infection, surgery, radioiodine and medications. It is potentially life-threatening. Features include tachycardia, heart failure, hyperthermia, extreme anxiety, altered mental state and gastrointestinal upset. Scoring systems have been developed in adults to aid diagnosis and can be helpful but have not been validated in children.
Treatment is with combination therapy: carbimazole (above dose, BNFC), beta-blocker (BNFC), iodide with iodine (potassium iodide (BNFC) and hydrocortisone (2 - 4 mg/kg 6 hourly IV, max 100mg per dose). Carbimazole is given 1 hour before potassium iodide to stop release of pre-formed hormone. Consider PHDU/ PICU admission and discussion with paediatric cardiology.
Treatment is with combination therapy: carbimazole (above dose, BNFC), beta-blocker (BNFC), iodide with iodine (potassium iodide (BNFC) and hydrocortisone (2 - 4 mg/kg 6 hourly IV, max 100mg per dose). Carbimazole is given 1 hour before potassium iodide to stop release of pre-formed hormone. Consider PHDU/ PICU admission and discussion with paediatric cardiology.
Process for Monitoring Compliance
The PIER network will review problems associated with this guideline through governance process.
Guideline to be reviewed after three years or sooner as a result of audit findings or as any changes to practice occurs.
Guideline to be reviewed after three years or sooner as a result of audit findings or as any changes to practice occurs.
References
- 2022 European Thyroid Association Guideline for the management of pediatric Graves' disease. CF Mooij, TD Cheetham, FA Verburg, A Eckstein, SH Pearce, J Léger, AS Paul van Trotsenburg. Eur Thyroid J. 2022;11(1):e210073
- Notes for the general paediatrician: managing thyrotoxicosis in children and young people. M Vidouris, C Worth, L Patel, A Date, A Jasser, B Hird, L Tetlow, I Banerjee. BMJ Paediatr Open. 2022;6(1):e001582
- 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. DS Ross, HB Burch, DS Cooper, MC Greenlee, P Laurberg, A Luiza Maia, SA Rivkees, MSamuels, J Sosa, MN Stan, MA Walter. Thyroid. 2016;26(10):1343-1421.
- Incidence of thyrotoxicosis in childhood: a national population based study in the UK and Ireland. Williamson S, Greene SA. Clin Endocrinol 2010;72:358–63.
|
Document Version:
1.0 Lead Authors: Prof. Justin Davies, Consultant Paediatric Endocrinologist, UHS Dr Vanessa Irvine, Consultant Paediatrician, St Richard's Hospital, Chichester |
Approving Network:
Wessex Paediatric Endocrinology Network Date of Approval: 05/2024 Review Due: 05/2027 |
PIER Contact |
|