Management of Henoch-Scholein Purpura (HSP) in Children

Introduction
Henoch-Schonlein purpura (HSP) is a multisystem disorder affecting mainly the skin, joints, gastro-intestinal tract and kidneys. Involvement of other organs (pulmonary haemorrage and CNS involvement) is rare. The extrarenal manifestations are due to a small vessel leukocytoclastic vasculitis. In the kidneys there is mesangial expansion with deposition of IgA. HSP can occur at any age but is most frequent in children under 10 years. There is a slight male predominance. The incidence is reported as 13.5-21.7/100,000 per year. It is more common in winter and commonly follows an upper respiratory infection. The aetiology and pathogenesis are poorly understood.
Henoch-Schonlein purpura (HSP) is a multisystem disorder affecting mainly the skin, joints, gastro-intestinal tract and kidneys. Involvement of other organs (pulmonary haemorrage and CNS involvement) is rare. The extrarenal manifestations are due to a small vessel leukocytoclastic vasculitis. In the kidneys there is mesangial expansion with deposition of IgA. HSP can occur at any age but is most frequent in children under 10 years. There is a slight male predominance. The incidence is reported as 13.5-21.7/100,000 per year. It is more common in winter and commonly follows an upper respiratory infection. The aetiology and pathogenesis are poorly understood.
Scope
This guideline is intended for use by all pediatricians within Wessex to guide the management of children presenting with suspected HSP.
This guideline is intended for use by all pediatricians within Wessex to guide the management of children presenting with suspected HSP.
Purpose
To aid in consistent management and follow up of HSP.
To aid in consistent management and follow up of HSP.
Features
HSP is a clinical diagnosis
HSP is a clinical diagnosis
|
Cutaneous
|

|
Gastrointestinal
Articular
Renal
Other features
- Occurs in 2/3 of cases (90% of those with renal involvement)
- Abdominal pain may preceed rash in 14-36% of patients
- Vomiting, diarrhoea, periumbilical pain, bloody stools, upper GIT haemorrhage
- Intussusception in 5% of patients
- Rarely: Haemorrhagic pancreatitis, hydrops of the gall bladder, pseudomembranous colitis
Articular
- 50-80% of patients
- Arthralgia, periarticular oedema
- Synovial effusions are typically absent
- Knees and ankles most commonly affected, less commonly wrists, fingers and elbows
Renal
- Present in 40-60%
- Renal involvement is often absent at presentation and may only be apparent weeks or months later
- Presentation of renal involvement is variable:
- Microscopic haematuria - transient or persistent
- Macroscopic haematuria
- Proteinuria
- Nephrotic syndrome
- Mixed nephritic-nephrotic syndrome
Other features
- Genital - Orchitis, cord haematoma, testicular pain or necrosis, painful ecchymotic induration of the scrotum
- CNS - Seizures, encephalopathy, coma, Guillian-Barre, cortical blindness, intracerebral haemorrhages, stroke
- Carditis
- Parotitis
- Pulmonary disease with heamorrhage
Differential Diagnosis
- Sepsis, especially meningococcal disease (see guideline for meningococcal disease)
- Systemic vasculitides (Wegeners, SLE, hypersentivity vasculitis, polyarteritis nodosa)
- ITP and other forms of purpura (see ITP guideline)
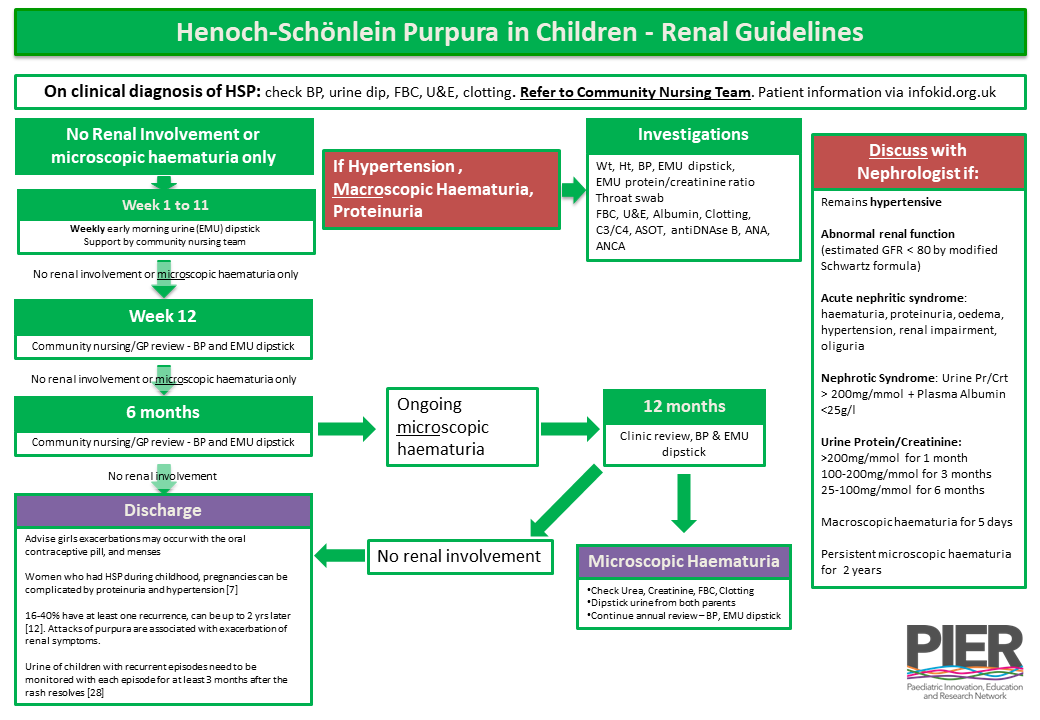
Initial Investigations
Other investigations are not routine if the patients is well, the clinical diagnosis is confident and the urine dipsticks are clear.
- Blood Pressure
- Urine Dipstick
- FBC, U&E, Clotting
Other investigations are not routine if the patients is well, the clinical diagnosis is confident and the urine dipsticks are clear.
Initial Management
- Supportive - Hydration, nutrition, electrolyte balance
- Simple analgesia - use non-steroidal anti-inflammatory agents only if the renal function is normal.
- If severe abdominal pain, arthritis, pulmonary haemorrhage - consider oral prednisolone 1-2mg/kg [1], [2] after discussion with consultant
- If severe skin manifestations - consider oral colchicine or oral dapsone [3], [4] in consultation with dermatologist
Consideration for Admission
Any patient with :
Any patient with :
- Severe joint pain
- Significant abdominal pain (as may have intussusception)
- Malaena
- Oedema/nephrotic syndrome
- Hypertension
Follow up
Treatment
Indications for referral to a paediatric nephrologist:
Renal Biopsy
Suggested treatment
Indications for referral to a paediatric nephrologist:
- Acute nephritic syndrome - haematuria, proteinuria, oedema, hypertensive, renal impairment, oliguria
- Macroscopic haematuria for 5 days
- Microscopic haematuria for 2 years
- Hypertension
- Proteinuria
- Nephrotic syndrome at any time
- Urine protein/creatinine ratio > 200 with normal plasma albumin concentration for 1 month
- Urine protein/creatinine ratio 100 to 200 for 3 months
- Urine protein/creatinine ratio 25 to 100 for 6 months
Renal Biopsy
- No firm evidence to guide us in the use
- Purpose - To confirm diagnosis, guide treatment, provide prognostic information
- Indications:
- Raised ASOT, abnormal C3/C4, ANCA, Auto antibody profile
- Rapidly progressive glomerulonephritis
- Acute nephritic syndrome [8],[9],[10]
- Nephrotic syndrome: 1 month after onset [5]
- Persistent nephrotic range proteinuria: 2 months after onset [11]
Suggested treatment
- Dialysis dependent rapidly progressive glomerulonephritis
- IV methylprednisolone 600mg/m2 once daily for 3 doses [18], [22]
- Plasma exchange [23]
- Cyclophosphamide PO (2.5mg/kg OD for 8 weeks) [18]
- (After 3 days of methylprednisolone) Prednisolone PO60mg/m2 once daily for 1 month, 40mg/m2 once daily for 1 month, then taper over the next 4 months (total 6 months)
- >50% Crescents
- IV Methylprednisolone 600 mg/m2 once daily for 3 doses [19], [22]
- Cyclophosphamide PO (2.5mg/kg once daily, 8wks) [18]
- (After 3 days of methylprednisolone) prednisolone PO 60mg/m2 once daily for 1 month, 40mg/m2 once daily for 1 month, then taper over next 4 month: total 6 months
- +/- Plasma exchange
- Crescents [18], [19], [20], [21], / Tubulo-interstitial changes [18], [19], [6]
- IV Methylprednisolone 600 mg/m2 once daily for 3 doses [19], [22], [26]
- +/- cyclophosphamide [22], [24], [25]
- (After 3 days of methylprednisolone) prednisolone PO 60mg/m2 once daily for 1 month, 40mg/m2 once daily for 1 month, then taper over next 4 months: total 6 months
+/- Plasma exchange
- Acute nephritic/ nephrotic syndrome with minimal biopsy findings [6], [21]
- Prednisolone PO 60mg/m2 once daily for 1 month, 40mg/m2 once daily for 1 month, then taper over next 4 months: total 6 months
- Consider adding Angiotensin converting enzyme inhibitors or Angiotensin II receptor antagonists
- Nephrotic range proteinuria
- Angiotensin converting enzyme Inhibitor / Angiotensin II receptor antagonists [Additional treatment dependent on biopsy findings]
- Persistent proteinuria (>100mg/mmol creatinine)
- Angiotensin converting enzyme inhibitor / Angiotensin II receptor antagonists [13], [14], [15], [16], [17]
References
[1] Allen DM, Diamond LK, Howell DA. Anaphylactoid purpura in children (Henoch-Schönlein syndrome). Am J Dis Child 1960; 99: 147-68
[2] Rosenblum ND, Winter HS. Steroid effects on the course of abdominal pain in children with HSP. Pediatr 1987; 79: 1018-21
[3] Fredenberg MF, Malkinson FD. Sulfone therapy in the treatment of
leukocytoclastic vasculitis. J Am Acad Dermatol 1987; 16: 772-78
Doc ID: 8916252d44adfa373198e3a29ab929fbf98450b9
[4] Hoffbrand BI. Dapsone in Henoch-Schönlein purpura-worth a trial? Postgrad Med 1991; 67: 961-62
[5] Ronkainen J, Ala-Houhala M, Huttunen –P, Jahnukainen T, Koskimies O, Örmälä T, Nuutinen M. Outcome of Henoch-Schönlein nephritis with nephritic range proteinuria. Clinical Nephrology 2003; 60(2): 80-84
[6] Foster BJ, Bernard C, Drummond KN, Sharma AK. Effective therapy for severe Henoch-Schönlein purpura nephritis with prednisolone and azathioprine: A clinical and histopathologic study. Journal of Pediatrics 2000;136(3): 370-375
[7] Ronkainen J, Nuutinen M, Koskimies O. The adult kidney 24 years after childhood Henoch-Schönlein purpura: a retrospective cohort study. Lancet 2002; 360(9334): 666-70
[8] Scharer K, Krmar R, Querfeld U, Ruder H, Waldherr R, Schaefer F. Clinicaloutcome of Henoch-Schönlein purpura nephritis in children. Pediatr Nephrol 1999;13(9): 816-23
[9] Coppo R, Mazzucco G, Cagnoli L, Lupo A, Schena FP. Long-term prognosis of Henoch-Schönlein nephritis in adults and children. Italian Group of Renal Immunopathology Collaborative Study on Henoch-Schönlein purpura. Nephrol Dial Transplant 1997; 12(11): 2277-83
[10] Stewart M, Savage JM, Bell B, McCord B. Long term renal prognosis of Henoch-Schönlein purpura in an unselected childhood population
[11] Andreoli SP. Chronic glomerulonephritis in childhood. Menbranoproliferative glomerulonephritis, Henoch-Schönlein purpura nephritis, and IgA nephropathy. Pediatr Clin North Am 1995; 42(6): 1487-503
[12] Saulsbury FT. Henoch-Schöenlein purpura in children. Report of 100 patients and review of the literature. Medicine 1999; 78: 395-409
[13] Woo KT, Lau YK, Wong KS, Chiang GSC. ACEI/ATRA therapy decreases proteinuria by improving glomerular permselectivity in IgA nephritis. Kidney International 2000; 58: 2485-2491
[14] Russo D, Pisani A, Balletta MM, De Nicola L, Savino FA, Andreucci M, Minutolo R. Additive antiproteinuric effect of converting enzyme inhibitor and Losartan in normotensive patients with IgA nephropathy. Am J Kidney Dis 1999; 33: 851-856
[15] Ruggenenti P, Perua A, Benini R, Bertani T, Zoccali C, Maggiore Q, Salvadori M, Remuzzi G. In chronic nephropathies prolonged ace inhibition can induce remission: Dynamics of time-dependent changes in GFR. J Am Soc Nephrol 1999; 10: 997-1006
[16] Nakamura t, Obata J, Kimura H, Ohno S, Yoshida Y, Kawaihi H, Schimizu F. Blocking angiotensin II ameliorates proteinuria and glomerular lesions in progressive mesangioproliferative glomeerulonephritis. Kidney Int 1999; 55: 877-889
[17] Nakajima M, Hutchinson HG, Fujinaga M, Hayashida W, Morishita R, Zhang L, Horiuchi M, Pratt RE, Dzau VJ. The angiotensin II type 2 (AT2) receptor antagonizes the growth effects of the AT1 receptor: Gain-of-function study using gene transfer. Proc Natl Acad Sci USA 1995; 92: 10663-10667 Doc ID: 8916252d44adfa373198e3a29ab929fbf98450b9
[18] Öner A, Tinaztepe K, Erdogan Ö. The effect of triple therapy on rapidly progressive type of Henoch-Schönlein nephritis. Pediatr Nephrol 1995; 9: 6-10
[19] Kawasaki Y, Suzuki J, Nozawa R, Suzuki S, Suzuki H. Efficacy of
methylprednisolone and urokinase pulse therapy for severe Henoch-Schönlein nephritis. Pediatrics 2003; 111(4): 785-789
[20] Jardim HM, Leake J, Risdon RA, Barratt TM, Dillon MJ. Crescentic
glomerulonephritis in children. Pediatr Nephrol 1992; 6(3): 231-5
[21] Bergstein J, Leiser J, Andreoli P. Response of crescentic Henoch-Schönlein purpura nephritis to corticosteroid and azathioprine therapy. Clinical Nephrology 1998; 49(1): 9-14
[22] Niaudet P, Habib R. Methylprednisolone pulse therapy in the treatment of severe forms of Schönlein-Henoch purpura nephritis. Pediatr Nephrol 1998; 12: 238-243
[23] Hattori M, Ito K, Konomoto T, Kawaguchi H, Yoshioka T, Khono M.
Plasmapheresis as the sole therapy for rapidly progressive Henoch-Schönlein purpura nephritis in children. American Journal of Kidney Diseases 1999; 33(3): 427-433
[24] Iijima K, Ito-Kariya S, Nakamura H, Yoshikawa N. Multiple combined therapy for severe Henoch-Schönlein nephritis in children. Pediatr Nephrol 1998; 12: 244-248
[25] Flynn JT, Smoyer WE, Bunchman TE, Kershaw DB, Sedman AB. Treatment of Henoch-Schönlein purpura glomerulonephritis in children with high-dose corticosteroids plus oral cyclophosphamide. Am J Nephrol 2001; 21: 128-133
[1] Allen DM, Diamond LK, Howell DA. Anaphylactoid purpura in children (Henoch-Schönlein syndrome). Am J Dis Child 1960; 99: 147-68
[2] Rosenblum ND, Winter HS. Steroid effects on the course of abdominal pain in children with HSP. Pediatr 1987; 79: 1018-21
[3] Fredenberg MF, Malkinson FD. Sulfone therapy in the treatment of
leukocytoclastic vasculitis. J Am Acad Dermatol 1987; 16: 772-78
Doc ID: 8916252d44adfa373198e3a29ab929fbf98450b9
[4] Hoffbrand BI. Dapsone in Henoch-Schönlein purpura-worth a trial? Postgrad Med 1991; 67: 961-62
[5] Ronkainen J, Ala-Houhala M, Huttunen –P, Jahnukainen T, Koskimies O, Örmälä T, Nuutinen M. Outcome of Henoch-Schönlein nephritis with nephritic range proteinuria. Clinical Nephrology 2003; 60(2): 80-84
[6] Foster BJ, Bernard C, Drummond KN, Sharma AK. Effective therapy for severe Henoch-Schönlein purpura nephritis with prednisolone and azathioprine: A clinical and histopathologic study. Journal of Pediatrics 2000;136(3): 370-375
[7] Ronkainen J, Nuutinen M, Koskimies O. The adult kidney 24 years after childhood Henoch-Schönlein purpura: a retrospective cohort study. Lancet 2002; 360(9334): 666-70
[8] Scharer K, Krmar R, Querfeld U, Ruder H, Waldherr R, Schaefer F. Clinicaloutcome of Henoch-Schönlein purpura nephritis in children. Pediatr Nephrol 1999;13(9): 816-23
[9] Coppo R, Mazzucco G, Cagnoli L, Lupo A, Schena FP. Long-term prognosis of Henoch-Schönlein nephritis in adults and children. Italian Group of Renal Immunopathology Collaborative Study on Henoch-Schönlein purpura. Nephrol Dial Transplant 1997; 12(11): 2277-83
[10] Stewart M, Savage JM, Bell B, McCord B. Long term renal prognosis of Henoch-Schönlein purpura in an unselected childhood population
[11] Andreoli SP. Chronic glomerulonephritis in childhood. Menbranoproliferative glomerulonephritis, Henoch-Schönlein purpura nephritis, and IgA nephropathy. Pediatr Clin North Am 1995; 42(6): 1487-503
[12] Saulsbury FT. Henoch-Schöenlein purpura in children. Report of 100 patients and review of the literature. Medicine 1999; 78: 395-409
[13] Woo KT, Lau YK, Wong KS, Chiang GSC. ACEI/ATRA therapy decreases proteinuria by improving glomerular permselectivity in IgA nephritis. Kidney International 2000; 58: 2485-2491
[14] Russo D, Pisani A, Balletta MM, De Nicola L, Savino FA, Andreucci M, Minutolo R. Additive antiproteinuric effect of converting enzyme inhibitor and Losartan in normotensive patients with IgA nephropathy. Am J Kidney Dis 1999; 33: 851-856
[15] Ruggenenti P, Perua A, Benini R, Bertani T, Zoccali C, Maggiore Q, Salvadori M, Remuzzi G. In chronic nephropathies prolonged ace inhibition can induce remission: Dynamics of time-dependent changes in GFR. J Am Soc Nephrol 1999; 10: 997-1006
[16] Nakamura t, Obata J, Kimura H, Ohno S, Yoshida Y, Kawaihi H, Schimizu F. Blocking angiotensin II ameliorates proteinuria and glomerular lesions in progressive mesangioproliferative glomeerulonephritis. Kidney Int 1999; 55: 877-889
[17] Nakajima M, Hutchinson HG, Fujinaga M, Hayashida W, Morishita R, Zhang L, Horiuchi M, Pratt RE, Dzau VJ. The angiotensin II type 2 (AT2) receptor antagonizes the growth effects of the AT1 receptor: Gain-of-function study using gene transfer. Proc Natl Acad Sci USA 1995; 92: 10663-10667 Doc ID: 8916252d44adfa373198e3a29ab929fbf98450b9
[18] Öner A, Tinaztepe K, Erdogan Ö. The effect of triple therapy on rapidly progressive type of Henoch-Schönlein nephritis. Pediatr Nephrol 1995; 9: 6-10
[19] Kawasaki Y, Suzuki J, Nozawa R, Suzuki S, Suzuki H. Efficacy of
methylprednisolone and urokinase pulse therapy for severe Henoch-Schönlein nephritis. Pediatrics 2003; 111(4): 785-789
[20] Jardim HM, Leake J, Risdon RA, Barratt TM, Dillon MJ. Crescentic
glomerulonephritis in children. Pediatr Nephrol 1992; 6(3): 231-5
[21] Bergstein J, Leiser J, Andreoli P. Response of crescentic Henoch-Schönlein purpura nephritis to corticosteroid and azathioprine therapy. Clinical Nephrology 1998; 49(1): 9-14
[22] Niaudet P, Habib R. Methylprednisolone pulse therapy in the treatment of severe forms of Schönlein-Henoch purpura nephritis. Pediatr Nephrol 1998; 12: 238-243
[23] Hattori M, Ito K, Konomoto T, Kawaguchi H, Yoshioka T, Khono M.
Plasmapheresis as the sole therapy for rapidly progressive Henoch-Schönlein purpura nephritis in children. American Journal of Kidney Diseases 1999; 33(3): 427-433
[24] Iijima K, Ito-Kariya S, Nakamura H, Yoshikawa N. Multiple combined therapy for severe Henoch-Schönlein nephritis in children. Pediatr Nephrol 1998; 12: 244-248
[25] Flynn JT, Smoyer WE, Bunchman TE, Kershaw DB, Sedman AB. Treatment of Henoch-Schönlein purpura glomerulonephritis in children with high-dose corticosteroids plus oral cyclophosphamide. Am J Nephrol 2001; 21: 128-133
|
Document Version:
1.0 Lead Author: Dr Shuman Haq, Consultant Nephrologist, UHS Additional Authors: Dr James Edelman, Paediatric Consultant, UHS |
Approving Network:
Wessex Nephrology Network Date of Approval: 26/8/19 Review Date: August 2022 |
PIER Contact |
|