Fever in babies less than 90 days old
Introduction
This aim of this pathway is to aid the assessment and management of infants below 90 days (≤28 and 29-90 days) who present to acute paediatric services with fever. National guidance is clear that there is an increased risk of bacterial infection in the neonatal group up to 28 days old and as such a rapid assessment and administration of antibiotics is required1. In those infants who are between 29-90 days old and are clinically well, a more staggered approach should be used, particularly in the context of the post-immunisation cohort.
Scope & Purpose
This guidance aims to ensure that the correct investigations are sent at the correct time which will help with ongoing management of these children under the care of paediatrics. The key role for the assessing team in the acute setting is early identification and acquisition of key samples prior to prompt delivery of antibiotics if appropriate.
This aim of this pathway is to aid the assessment and management of infants below 90 days (≤28 and 29-90 days) who present to acute paediatric services with fever. National guidance is clear that there is an increased risk of bacterial infection in the neonatal group up to 28 days old and as such a rapid assessment and administration of antibiotics is required1. In those infants who are between 29-90 days old and are clinically well, a more staggered approach should be used, particularly in the context of the post-immunisation cohort.
Scope & Purpose
This guidance aims to ensure that the correct investigations are sent at the correct time which will help with ongoing management of these children under the care of paediatrics. The key role for the assessing team in the acute setting is early identification and acquisition of key samples prior to prompt delivery of antibiotics if appropriate.
Definitions
Fever: Documented temperature ≥38°C
FBC: Full blood Count
U&E: Urea and Electrolytes
CRP: C-reactive protein
CSF: Cerebrospinal fluid
LP: Lumbar puncture
FBC: Full blood Count
U&E: Urea and Electrolytes
CRP: C-reactive protein
CSF: Cerebrospinal fluid
LP: Lumbar puncture
Guideline
Any documented fever ≥38°C in a baby < 90 days is concerning and will often be accompanied by features in the history and examination that would support a diagnosis of infection. All babies should receive sepsis screening as per standard protocol. Any baby who screens positive should be treated accordingly as per the paediatric sepsis 6. Of those who appear well, the clinician should ascertain the methods by which the temperature was obtained. If this was using a digital axillary thermometer, including at home, then progression down the pathway should be commenced (Appendix A). If the infant appears well and the temperature was recorded by other means, there is a role for close observation within the department with escalation as required should they develop a fever or become unwell.
In those aged 28 days or less with a documented fever ≥38°C on digital axillary thermometer a full panel of investigations including FBC, U&E, CRP, coagulation profile and a blood gas for lactate as well as urine, blood and CSF cultures should be performed and IV antibiotics given without delay.
Infants 29 days and above days of age with no concerning features on assessment should have bloods taken (FBC, U&E, CRP, culture if starting IV antibiotics) and a urine sample collected, preferably by in/out catheter with timely review of the results along with continuing observation guiding management (note: if fever within 24 hours of vaccines and feeding well/handing well, can hold off bloods/urine and safety net if no other concerns – see below). It is safe to manage some low-risk infants without routine lumbar puncture or empirical antibiotics.2 It is important to remember that not all babies with sepsis present with fever.
Fever post immunisations: At or around 8 weeks of age the routine infant immunisation schedule begins, including the Meningococcal B vaccine (Bexsero), which is known to be highly pyrogenic. It may be appropriate to manage infants who are otherwise well appearing and develop a fever within 48hrs of their 8 week immunisations with watchful waiting only and discharged with high quality safety net advice.
Bronchiolitis: Senior clinician discretion can be applied in the setting of clinical bronchiolitis in the presence of fever in those >28 days.
Acquiring cultures: Sending samples for blood and urine culture prior to antibiotics administration is essential. At least 0.5ml of blood is required for culture.
Urine: Due to high rates of contamination with clean catch urine, urine collection is ideally achieved by in/out catheterisation. Urinalysis has good sensitivity and specificity in infants for detecting urinary tract infections.(3)
Neonatal swabs: These are swabs taken from the eyes, throat and rectum in Viral Transport Medium (green swabs) and can be helpful in identifying a viral cause for the symptoms which can help with rationalising antibiotic use.
Chest X-ray: An early sign in children and babies when they are unwell is a raised respiratory rate. A chest X-ray is not part of the initial septic screen for a baby unless there are clear chest signs or features to consider a respiratory focus of infection.
CSF: All infants ≤28 days of age or who are ill appearing should have a lumbar puncture performed. This should only be done if there are no contraindications as described below. Consider an LP in infants with equivocal signs or symptoms and raised inflammatory markers. Use of WCC to guide need for lumbar puncture is not recommended. (4, 5) Samples should be sent for biochemical analysis of glucose and protein. Microbiology samples for MC&S, culture and viral PCRs should be sent.
Table 1 - CSF Sample collection guide
In those aged 28 days or less with a documented fever ≥38°C on digital axillary thermometer a full panel of investigations including FBC, U&E, CRP, coagulation profile and a blood gas for lactate as well as urine, blood and CSF cultures should be performed and IV antibiotics given without delay.
Infants 29 days and above days of age with no concerning features on assessment should have bloods taken (FBC, U&E, CRP, culture if starting IV antibiotics) and a urine sample collected, preferably by in/out catheter with timely review of the results along with continuing observation guiding management (note: if fever within 24 hours of vaccines and feeding well/handing well, can hold off bloods/urine and safety net if no other concerns – see below). It is safe to manage some low-risk infants without routine lumbar puncture or empirical antibiotics.2 It is important to remember that not all babies with sepsis present with fever.
Fever post immunisations: At or around 8 weeks of age the routine infant immunisation schedule begins, including the Meningococcal B vaccine (Bexsero), which is known to be highly pyrogenic. It may be appropriate to manage infants who are otherwise well appearing and develop a fever within 48hrs of their 8 week immunisations with watchful waiting only and discharged with high quality safety net advice.
Bronchiolitis: Senior clinician discretion can be applied in the setting of clinical bronchiolitis in the presence of fever in those >28 days.
Acquiring cultures: Sending samples for blood and urine culture prior to antibiotics administration is essential. At least 0.5ml of blood is required for culture.
Urine: Due to high rates of contamination with clean catch urine, urine collection is ideally achieved by in/out catheterisation. Urinalysis has good sensitivity and specificity in infants for detecting urinary tract infections.(3)
Neonatal swabs: These are swabs taken from the eyes, throat and rectum in Viral Transport Medium (green swabs) and can be helpful in identifying a viral cause for the symptoms which can help with rationalising antibiotic use.
Chest X-ray: An early sign in children and babies when they are unwell is a raised respiratory rate. A chest X-ray is not part of the initial septic screen for a baby unless there are clear chest signs or features to consider a respiratory focus of infection.
CSF: All infants ≤28 days of age or who are ill appearing should have a lumbar puncture performed. This should only be done if there are no contraindications as described below. Consider an LP in infants with equivocal signs or symptoms and raised inflammatory markers. Use of WCC to guide need for lumbar puncture is not recommended. (4, 5) Samples should be sent for biochemical analysis of glucose and protein. Microbiology samples for MC&S, culture and viral PCRs should be sent.
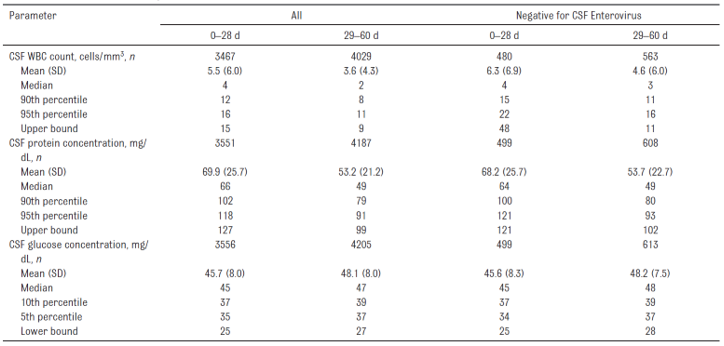
Table 1 - CSF Sample collection guide

Normal CSF ranges for babies <2 months of age
As interpretation the following table taken from Thompson J el al. Paediatrics Volume 141, number 3, March 2018 suggests that using 90th percentile as upper limit of normal. For glucose: mg/dl = 18 × mmol/l. (6)
Note due to sensitive PCR testing and WCC interpretation acquisition of the CSF sample prior to giving antibiotics is less key than urine and blood and should not delay administering IV Abx. Contra-indications to LP include signs of shock, Plts <100, abnormal clotting, a spreading meningococcal rash and infection at the LP site.(7)
As interpretation the following table taken from Thompson J el al. Paediatrics Volume 141, number 3, March 2018 suggests that using 90th percentile as upper limit of normal. For glucose: mg/dl = 18 × mmol/l. (6)
Note due to sensitive PCR testing and WCC interpretation acquisition of the CSF sample prior to giving antibiotics is less key than urine and blood and should not delay administering IV Abx. Contra-indications to LP include signs of shock, Plts <100, abnormal clotting, a spreading meningococcal rash and infection at the LP site.(7)
Antibiotics: For all babies ≤28 days old with confirmed fever, commence IV antibiotics as per microguide. For infants between 29 and 90 days, commence antibiotics if clinically unwell, if urinalysis is suggestive of urinary tract infection, or inflammatory markers are significantly elevated (CRP >20). If there are signs of sepsis with shock, antibiotics must be administered within one hour. If there are no signs of shock present, aim to commence antibiotics within 3 hours. Perform LP if positive blood culture (non-contaminant) in absence of focus of infection.
Resources and Staffing: For babies in this pathway there is a spectrum of severity which includes the collapsed neonate and there is further guidance available on the SORT website as well as PIER network for managing those patients who are very well. Early escalation to senior ED colleagues, the Consultant General Paediatrician and PICU as required is entirely appropriate.
Ambulation: In some cases, babies aged <3 months of age with fever can be ambulated on IV antibiotics following a brief period of observation (4 hours). The babies will need referral to the ambulatory OPAT clinic to ensure follow-up and further doses of antibiotics if required.
Summary: Early identification and management of infants <3 months with signs of sepsis is key as well as judicious use of antibiotics. It is therefore vital to have a robust policy in place for those presenting with fever. It is however also vital to reiterate that babies with underlying sepsis can present without fever and a low threshold should be in place for investigation and commencement of IV Antibiotics in those with altered haemodynamic or neurological state. Prioritisation of acquiring blood and urine cultures before prompt administration of systemic antibiotics where indicated is key, as well as opting for a period of observation awaiting further results in those older infants presenting with fever in isolation.
Acute paediatric teams have an important role to play acquiring key microbiological samples before deciding if treatment is required. Once on IV antibiotics decisions can be made regarding the appropriateness of ambulation as per local trust protocol.
Resources and Staffing: For babies in this pathway there is a spectrum of severity which includes the collapsed neonate and there is further guidance available on the SORT website as well as PIER network for managing those patients who are very well. Early escalation to senior ED colleagues, the Consultant General Paediatrician and PICU as required is entirely appropriate.
Ambulation: In some cases, babies aged <3 months of age with fever can be ambulated on IV antibiotics following a brief period of observation (4 hours). The babies will need referral to the ambulatory OPAT clinic to ensure follow-up and further doses of antibiotics if required.
Summary: Early identification and management of infants <3 months with signs of sepsis is key as well as judicious use of antibiotics. It is therefore vital to have a robust policy in place for those presenting with fever. It is however also vital to reiterate that babies with underlying sepsis can present without fever and a low threshold should be in place for investigation and commencement of IV Antibiotics in those with altered haemodynamic or neurological state. Prioritisation of acquiring blood and urine cultures before prompt administration of systemic antibiotics where indicated is key, as well as opting for a period of observation awaiting further results in those older infants presenting with fever in isolation.
Acute paediatric teams have an important role to play acquiring key microbiological samples before deciding if treatment is required. Once on IV antibiotics decisions can be made regarding the appropriateness of ambulation as per local trust protocol.
Communication & Training Plans
Guideline will be made available on the PIER website, dissemination and raised awareness can occur via clinical leads at each centre
Process for Monitoring Compliance
The purpose of monitoring is to provide assurance that the agreed approach is being followed. This ensures that we get things right for patients, use resources well and protect our reputation. Our monitoring will therefore be proportionate, achievable and deal with specifics that can be assessed or measured
References
- NICE guidance on Fever under five: assessment and initial management: found at URL:https://www.nice.org.uk/guidance/ng143/chapter/Recommendations#management - by-the-paediatric-specialist.
- Giulia Trippella, Luisa Galli, Maurizio De Martino, Catiuscia Lisi & Elena Chiappini (2017) Procalcitonin performance in detecting serious and invasive bacterial infections in children with fever without apparent source: a systematic review and meta-analysis, Expert Review of Anti-infective Therapy, 15:11, 1041- 1057, DOI: 10.1080/14787210.2017.1400907
- Accuracy of the Urinalysis for Urinary Tract Infections in Febrile Infants 60 Days and Younger Leah Tzimenatos, Prashant Mahajan, Peter S. Dayan, Melissa Vitale, James G. Linakis, Stephen Blumberg, Dominic Borgialli, Richard M. Ruddy, John Van Buren, Octavio Ramilo, Nathan Kuppermann and for the Pediatric Emergency Care Applied Research Network (PECARN):
- De S, Williams GJ, Hayen A, et al. Value of white cell count in predicting serious bacterial infection in febrile children under 5 years of age. Archives of Disease in Childhood 2014;99:493-499
- Gomez B, Mintegi S, Bressan S, et al. Validation of the "Step-by-Step" Approach in the Management of Young Febrile Infants. Pediatrics. 2016;138(2):e20154381. doi:10.1542/peds.2015-4381
- Nutrient Intake in the First Two Weeks of Life and Brain Growth in Preterm Neonates. Juliane Schneider, Céline J. Fischer Fumeaux, Emma G. Duerden, Ting Guo, Justin Foong, Myriam Bickle Graz, Patric Hagmann, M. Mallar Chakravarty, Petra S. Hüppi, Lydie Beauport, Anita C. Truttmann and Steven P. Miller. Pediatrics March 2018, 141 (3) e20172169; DOI: https://doi.org/10.1542/peds.2017-2169.
- PIER guideline Management of suspected meningitis URL: http://www.pier.uhs.nhs.uk/Media/Guidelines/Management-of-suspected-meningitisguideline.pdf 8) Surviving sepsis campaign guideline. URL: https://journals.lww.com/pccmjournal/fulltext/2020/02000/surviving_sepsis_campaign _international_guidelines.20.aspx
|
Document Version:
1.0 Lead Authors: R. King (Paediatric Registrar) L. Anthony (Paediatric Registrar) D. James (PEM Consultant, UHS) S. Patel (Infectious Diseases Consultant, UHS) |
Approving Network:
Wessex Paediatric Emergency Medicine Network Wessex Infectious Diseases Network Date of Approval: June 2023 Review Due: June 2026 |
PIER Contact |
|