Haematuria in Children
Flowchart
Introduction
Haematuria may be an important sign of urinary tract and renal disease. Healthy children can have occasional red cells in the urine but persistent microscopic haematuria is considered significant if there are > 10 red cells/high power field in at least 3 fresh samples collected a minimum of 1 week apart.
Haematuria can be gross (i.e. the urine is overtly bloody, smoky, or tea coloured) or microscopic, symptomatic or asymptomatic, transient or persistent, and either isolated or associated with other urinary abnormalities such as proteinuria. Gross or macroscopic haematuria deserves prompt investigation to determine its cause. The degree of haematuria bears no relationship to the seriousness of the underlying cause. It may be initial (suggesting a urethral cause); total/complete (due to kidney or diffuse bladder pathology) or terminal (in prostatic, trigonal or posterior urethral disorders).
Substances other than red blood cells can cause the urine to become red in colour (see table 1).
Haematuria can be gross (i.e. the urine is overtly bloody, smoky, or tea coloured) or microscopic, symptomatic or asymptomatic, transient or persistent, and either isolated or associated with other urinary abnormalities such as proteinuria. Gross or macroscopic haematuria deserves prompt investigation to determine its cause. The degree of haematuria bears no relationship to the seriousness of the underlying cause. It may be initial (suggesting a urethral cause); total/complete (due to kidney or diffuse bladder pathology) or terminal (in prostatic, trigonal or posterior urethral disorders).
Substances other than red blood cells can cause the urine to become red in colour (see table 1).
Scope
This guideline applies to all paediatric patients in the region other than neonates.
Purpose
The purpose of this guideline is to provide a standardised approach to the management of haematuria. These guidelines are aimed at providing the doctors presented with a child with haematuria with information to help identify the underlying problem and to guide management.
Definitions
Microscopic haematuria is considered significant if there are greater than 10 red cells/high power field in at least 3 fresh samples collected a minimum of 1 week apart. There is no published data detailing the number of RBCs seen on microscopy for each dipstick result. However, 1+ or greater on repeated samples is regarded as significant. Note that red blood cells lyse rapidly in dilute or acidic urine and so negative microscopy for red blood cells is only valid if performed promptly on a freshly voided specimen.
Macroscopic haematuria is where the urine is visibly discoloured. As little as 1mL of blood per litre of urine can produce a visible change in the urine colour.
Macroscopic haematuria is where the urine is visibly discoloured. As little as 1mL of blood per litre of urine can produce a visible change in the urine colour.
|
EMU - Early morning urine
GN - Glomerulonephritis ASOT - antistreptolysin O titre; U&E - urea and electrolytes FBC - full blood count USS - ultrasound XR KUB - x-ray kidneys/ureters/bladder Hb - haemoglobin HSP - Henoch-Schönlein purpura |
FSGS - focal segmental glomerulosclerosis
ANCA - Antineutrophil cytoplasmic antibodies ANA -Antinuclear antibodies ESR - Erythrocyte sedimentation rate LDH - Lactate dehydrogenase ADPKD - Autosomal dominant polycystic kidney disease ARPKD - Autosomal recessive PKD PCR - protein:creatinine ratio |
Causes of Haematuria and Relevant Investigations
Lower urinary tract blood will be red or pink coloured and may be at the beginning or end of micturition. Glomerular haematuria can be red, pink or cola coloured due to longer contact with the acidic urine causing the haem pigment to be oxidised to a methaem derivative. Dysmorphic red blood cells and acanthocytes can be seen on urine microscopy.
Not all red urine is haematuria. Refer to table 1 for non-haematuria causes of red urine. Exogenous blood, as with contamination with menstruation or in fabricated or induced illness (FII) should also be considered. Please refer to the Royal College of Paediatrics and Child Health (RCPCH) child protection companion for advice on recognition and management.
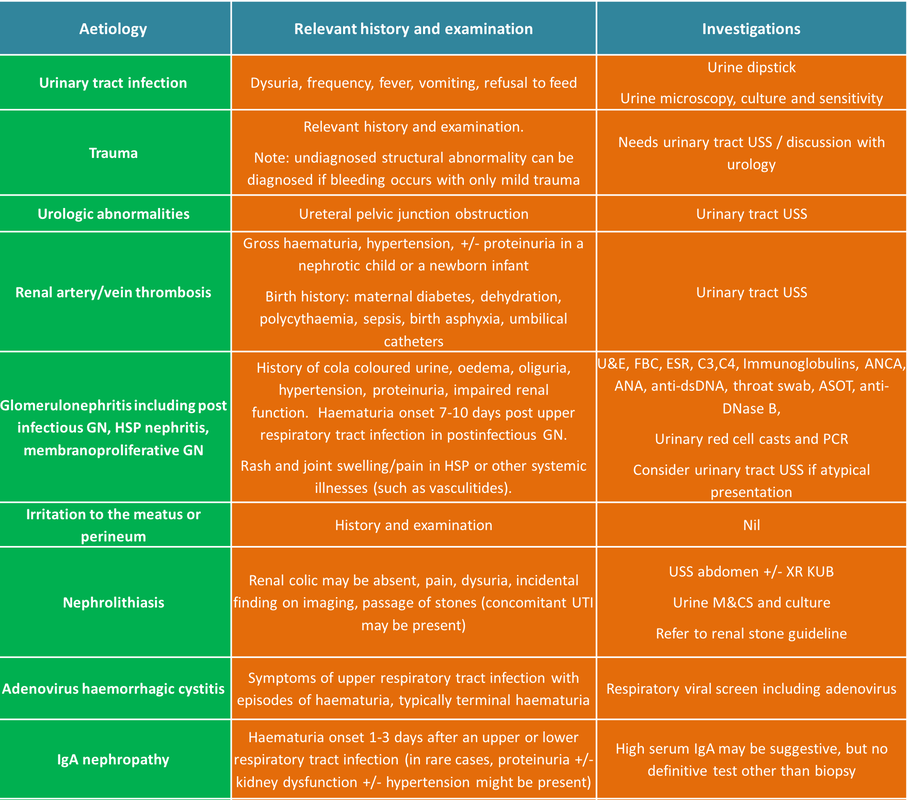
Haematuria has a range of causes and investigations depending on the relevant history and examination. Potential causes of microscopic haematuria are listed in Table 2 and microscopic and/or macroscopic haematuria are listed in Table 3.
Macroscopic Haematuria
Not all red urine is haematuria. Refer to table 1 for non-haematuria causes of red urine. Exogenous blood, as with contamination with menstruation or in fabricated or induced illness (FII) should also be considered. Please refer to the Royal College of Paediatrics and Child Health (RCPCH) child protection companion for advice on recognition and management.
Haematuria has a range of causes and investigations depending on the relevant history and examination. Potential causes of microscopic haematuria are listed in Table 2 and microscopic and/or macroscopic haematuria are listed in Table 3.
Macroscopic Haematuria
Investigation of macroscopic haematuria can be targeted towards glomerular causes if the urine is dark, ‘tea’ or ‘cola’ coloured or towards lower urinary tract causes if red or pink. Moreover, the source of haematuria may be suggested by timing during micturition. Haematuria present throughout the urinary stream indicates bleeding anywhere along the urinary tract, whereas terminal hematuria indicates a bladder or urethral origin. Blood clots and dysuria are also suggestive of lower urinary tract pathology.
Microscopic Haematuria
Microscopic Haematuria
Transient microscopic haematuria in children is common, particularly in association with intercurrent illness, but requires more thorough investigation and referral is indicated in certain cases.
A patient with a finding of microscopic haematuria should be screened for hypertension and proteinuria. Parents’ urine should also be checked for blood and parents asked about a family history of familial haematuria, early onset kidney failure, hearing loss or recurrent gross haematuria. In many cases microscopic haematuria is transient and the patient can be discharged from further follow up if subsequent urine samples are clear of blood and no other abnormalities identified. If microscopic haematuria is persistent further investigations are indicated as outlined in the flowcharts including screening for microalbuminuria.
Patients should have outpatient follow up at a suggested frequency in uncomplicated microscopic haematuria of 4 monthly for the first year and then annually. Check blood pressure, urine dip and albumin:creatinine ratio on an early morning urine sample at each visit. Cases can be discussed with the local nephro-urology lead with a view to referral to the paediatric nephrology team for persistent haematuria beyond one year or sooner if a diagnosis of familial haematuria is confirmed. This is summarised in the flowchart below.
In the event of familial haematuria or Alport syndrome being suspected all first-degree relatives should be screened for haematuria with affected adults referred to their General Practitioner and affected siblings referred to the paediatric nephrology team. Genetic testing may be appropriate in this scenario.
A patient with a finding of microscopic haematuria should be screened for hypertension and proteinuria. Parents’ urine should also be checked for blood and parents asked about a family history of familial haematuria, early onset kidney failure, hearing loss or recurrent gross haematuria. In many cases microscopic haematuria is transient and the patient can be discharged from further follow up if subsequent urine samples are clear of blood and no other abnormalities identified. If microscopic haematuria is persistent further investigations are indicated as outlined in the flowcharts including screening for microalbuminuria.
Patients should have outpatient follow up at a suggested frequency in uncomplicated microscopic haematuria of 4 monthly for the first year and then annually. Check blood pressure, urine dip and albumin:creatinine ratio on an early morning urine sample at each visit. Cases can be discussed with the local nephro-urology lead with a view to referral to the paediatric nephrology team for persistent haematuria beyond one year or sooner if a diagnosis of familial haematuria is confirmed. This is summarised in the flowchart below.
In the event of familial haematuria or Alport syndrome being suspected all first-degree relatives should be screened for haematuria with affected adults referred to their General Practitioner and affected siblings referred to the paediatric nephrology team. Genetic testing may be appropriate in this scenario.
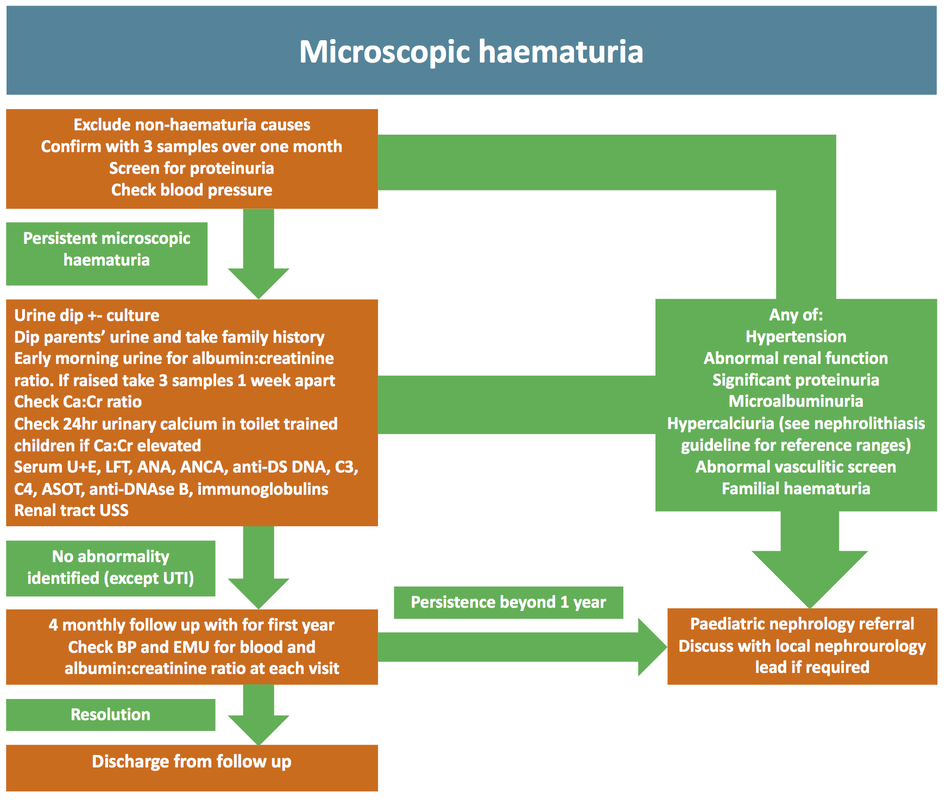
Table 1: Non-Haematuria Causes of Red or Brown Urine
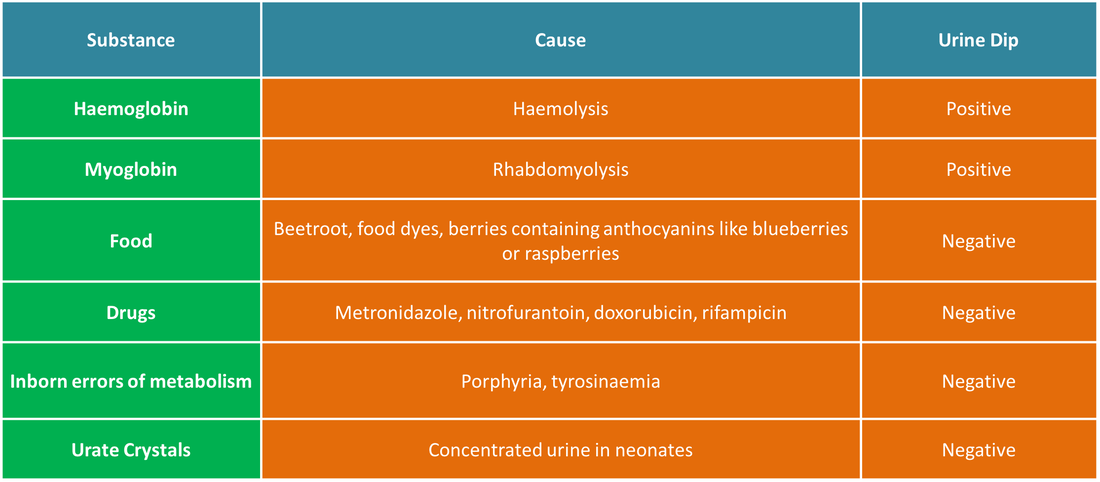
Table 2: Microscopic Haematuria Only
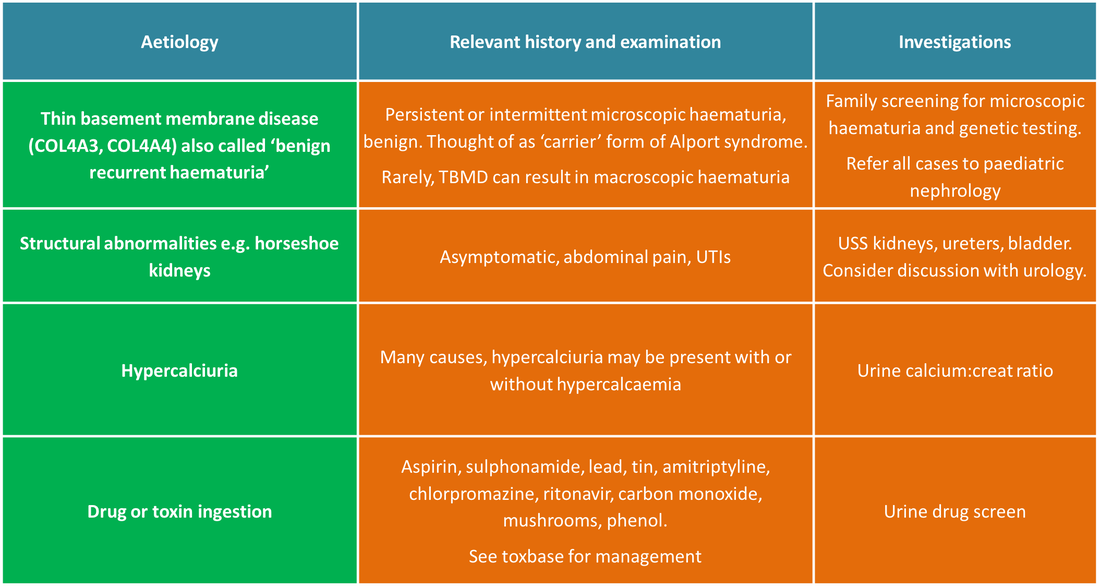
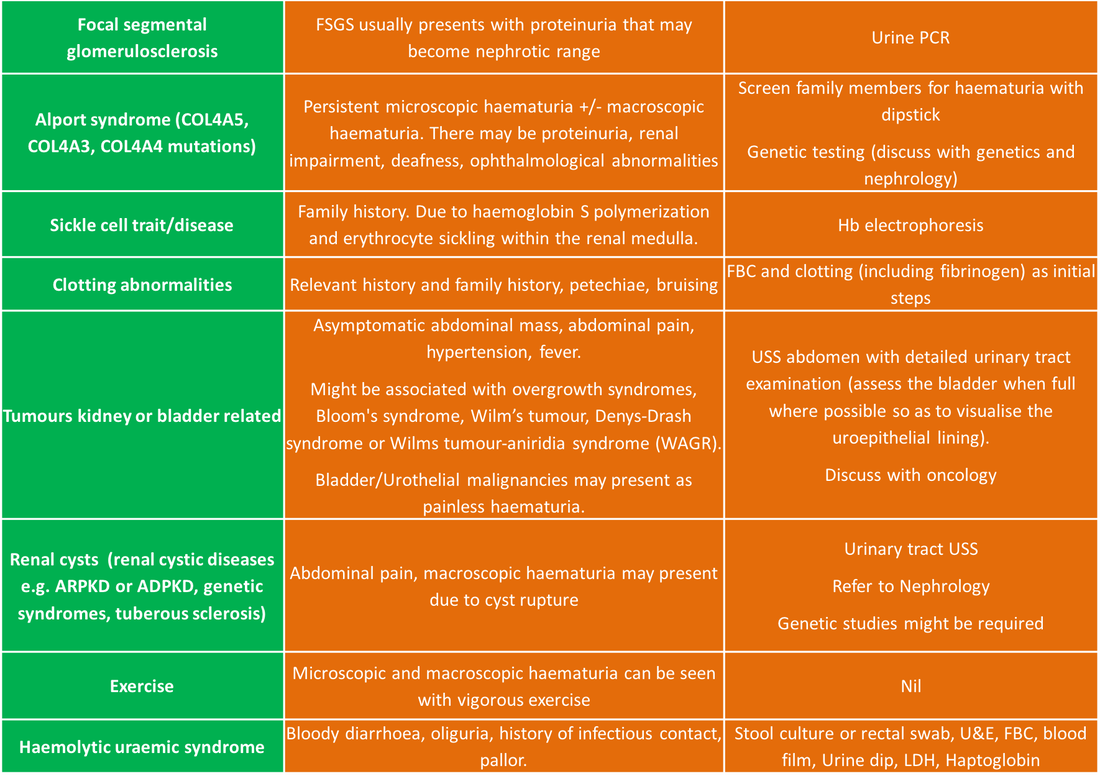
Table 3: Causes of Microscopic or Macroscopic Haematuria
Indications for Discussion with Paediatric Nephrology
- Hypertension (> 95th centile for age and height or >90th centile associated with proteinuria)
- Oliguria/anuria or signs of fluid overload
- Hyperkalaemia or abnormal renal function >5.5mmol/L
- Significant proteinuria (2+ on dipstick or greater, PCR>50mg/mmol) Immediate telephone consult if nephrotic range proteinuria of >200mg/mmol.
- Albumin:creatinine ratio above upper limit of normal for local laboratory on 3 consecutive occasions (samples one week apart)
- Atypical complement pattern- low C3 beyond 12 weeks or low C4 identified.
- Abnormal vasculitis screening
- Diagnosis of glomerulonephritis likely
- Persistent isolated microscopic haematuria
- Familial haematuria
- Macroscopic haematuria with no medical cause identified
- Hypercalciuria (refer to PIER nephrolithiasis and nephrocalcinosis guideline for reference rangesby age)
Implementation and Monitoring Effectiveness
This guideline will be made available regionally on the PIER Website. Local leads for paediatric nephrology will disseminate guideline and raise awareness locally.
The Paediatric Nephro-urology network will review problems associated with this guideline
through its governance process.
The Paediatric Nephro-urology network will review problems associated with this guideline
through its governance process.
References
- Balasubramanian R, marks SD. Post-infectious glomerulonephritis. Paediatr Int Child health2017; 37(4): 240-7
- Brown DD, Reidy KJ. Approach to the child with hematuria. Pediatr Clin North Am (2019);66(1): 15-30
- Clark M, Aronoff S, Del Vecchio M. Etiologies of asymptomatic microscopic hematuria in children - systematic review of 1092 subjects. Diagnosis (Berl) 2015;2(4):211–6.
- Coward RJ, Peters CJ, Duffy PG, et al. Epidemiology of paediatric renal stone disease in the UK. Arch Dis Child 2003; 88(11): 962-5
- Dalrymple RA, Ramage IJ. Fifteen-minute consultation: the management of microscopic haematuria. Arch Dis Child Educ Pract Ed (2017) Oct: 102(5): 230-234
- Gardner-Medwin JM, Dolezalova P, Cummins C et al. incidence of Henoch-Schonlein purpura, Kawasaki disease, and rare vasculitides in children of different ethnic origins. Lancet 2002;360(9341):1197-202
- Greenfield SP, Williot P, Kaplan, D. Gross hematuria in children: 1 ten-year review. Urology 2007; 69(1):166-9
- Hahn D, Hodson EM, Willis NS, et al. Interventions for preventing and treating kidney disease in Henoch-Schonlein Purpura (HSP). Cochrane Database Sys Rev 2015;(8):CD005128
- Harmon WE, Stablein D, Alexander SR, et al. Graft thrombosis in pediatric renal transplant recipients. A report of the North American Pediatric Renal Transplant Cooperative Study. Transplantation 1991;51(2):406–12.
- Kallash M, Rheault M. Approach to Persistent Microscopic Haematuria in Children. Kidney360 2020; 1:1014-1020
- Kuhle S, Massicotte P, Chan A, et al. A case series of 72 neonates with renal vein thrombosis. Data from the 1-800-NO-CLOTS registry. Thromb Haemost 2004; 92(4):729–33.
- Maillard N, Wyatt RJ, Julian BA, et al. Current understanding of the role of complement in IgA nephropathy. J Am Soc Nephrol 2015;26(7):1503-12
- Moudgil A. Renal venous thrombosis in neonates. Curr Pediatr Rev 2014;10(2): 101–6.
- Tinaztepe K, Buyan N, Tinaztepe B, et al. The association of nephrotic syndrome and renal vein thrombosis: a clinicopathological analysis of eight pediatric patients. Turk J Pediatr 1989;31(1):1–18.
- Vivante A, Afek A, Frenkel-Nir Y, et al. Persistent asymptomatic isolated microscopic hematuria in Israeli adolescents and young adults and risk for end stage renal disease. JAMA 2011;306(7):729–36.
- Wallis MC, Lorenzo AJ, Farhat WA, et al. Risk assessment of incidentally detected complex renal cysts in children: potential role for a modification of the Bosniak classification. J Urol 2008;180(1):317–21. 95. Akoh JA. Current management of autosomal dominant polycystic kidney disease. World J Nephrol 2015;4(4):468–79.
|
Document Version:
1.0 Lead Authors: Dr John Tolliday Approving Network: Wessex Nephrourology Network |
Date of Approval:
October 2021 Review Due:
October 2024 |
PIER Contact |
|