Paediatric Foreign Body Ingestion
Flowcharts
Hazardous or Symptomatic Ingested Foreign Body Algorithm
Management of Confirmed Button Battery on X-Ray
Non-Hazardous and Asymptomatic Ingested Foreign Body Algorithm
Introduction, Scope & Purpose
The ingestion of everyday objects is a frequently seen presentation to the Children’s Emergency Department (CED), with most cases occurring in children aged 6 months – 3 years.
The vast majority of foreign bodies will pass through the gastrointestinal tract without incident. However, some foreign bodies will cause harm such as:
This guidance should be used by any staff involved in the care of children aged 17 years and younger who have ingested a foreign body. This guidance does not cover the ingestion of absorbable toxic materials e.g. plants or chemicals, food boluses, or the ingestion of wrapped drugs (body packing/ body stuffing) – refer to TOXBASE for guidance on managing these conditions.
The aim of this document is to enable the standardised and safe management of ingested foreign bodies in children, and avoid unnecessary radiation.
This guidance outlines:
The vast majority of foreign bodies will pass through the gastrointestinal tract without incident. However, some foreign bodies will cause harm such as:
- Oesophageal obstruction
- Oesophageal perforation
- Fistulae into surrounding structures e.g. trachea, blood vessels
- Bowel obstruction
- Bowel perforation
This guidance should be used by any staff involved in the care of children aged 17 years and younger who have ingested a foreign body. This guidance does not cover the ingestion of absorbable toxic materials e.g. plants or chemicals, food boluses, or the ingestion of wrapped drugs (body packing/ body stuffing) – refer to TOXBASE for guidance on managing these conditions.
The aim of this document is to enable the standardised and safe management of ingested foreign bodies in children, and avoid unnecessary radiation.
This guidance outlines:
- Which patients can safely go home without investigation and without follow-up
- Which patients require investigations
- Which patients should be referred, and to which specialty
Definitions
Ingested Foreign Body (FB)
A non-absorbable object in the gastro-intestinal tract or lodged in the airway.
Hazardous Ingestion
Signs and symptoms a child may experience following ingestion of a foreign body.
Radiopaque
Structures which do not permit the passage of radiation and are therefore visible on X-ray. Structures which are radiopaque include:
Radiolucent
Structures which permit the passage of radiation and are not visible on x-ray, e.g. wood, plastic.
Button Batteries
Also known as “coin cells”, these coin shaped batteries are thin compared to their diameter. Diameter is typically 5-25mm. Commonly found in watches, hearing aids, some remote controls and toys.
Cylindrical and Rectangular Batteries
AA, AAA, 9V type batteries
A non-absorbable object in the gastro-intestinal tract or lodged in the airway.
Hazardous Ingestion
- Button Batteries and other batteries
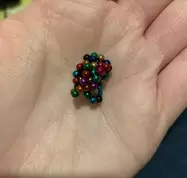
- Magnets e.g. ball bearings, magnetic false piercings
- Large Objects (length>6cm or width >2 cm)
- Sharp Object (including fish bones)
- Children with pre existing GI pathology
Signs and symptoms a child may experience following ingestion of a foreign body.
- Stridor, drooling, gagging
- Dysphagia, food refusal
- Sensation of FB, sore throat
- Cough, chest pain
- Abdominal pain, abdominal distension
- Vomiting
- Abnormal observations
Radiopaque
Structures which do not permit the passage of radiation and are therefore visible on X-ray. Structures which are radiopaque include:
- Metals e.g. coins, magnets, batteries
- Glass
- Stone/gravel
- Some fish bones e.g. cod, haddock, lemon sole, monkfish (contact radiology for full list)
Radiolucent
Structures which permit the passage of radiation and are not visible on x-ray, e.g. wood, plastic.
Button Batteries
Also known as “coin cells”, these coin shaped batteries are thin compared to their diameter. Diameter is typically 5-25mm. Commonly found in watches, hearing aids, some remote controls and toys.
Cylindrical and Rectangular Batteries
AA, AAA, 9V type batteries

Button Batteries
|

Cylindrical and Rectangular Batteries
|
Management of Hazardous and Symptomatic Ingestions
Most hazardous foreign bodies will be radiopaque and therefore visible on X-ray. Obtain a chest X-ray to visualise the location of the FB to enable referral to the correct specialty.
A foreign body visualised above the level of the clavicles suggests upper oesophageal obstruction and requires referral to ENT. A patient with a foreign body visualised below the level of the clavicles should be referred to paediatric surgery (if aged under 16 years) or adult endoscopy (16 or 17 years). However, in some regional centres ENT are able to remove foreign bodies further down the oesophagus, so consider discussing with your local ENT service as well as paediatric surgery.
If the FB is not seen on chest X-ray consider whether it could be more proximal or distal to what has been imaged and obtain a soft tissue neck and/or abdominal X-ray. Even if the FB is radiolucent and unlikely to be visualised on X-ray (e.g. a wooden toothpick), a chest X-ray is useful to exclude complications such as pneumomediastinum and pneumoperitoneum.
If the suspected foreign body is a radiopaque material, cannot be visualised on X-ray and the child is well, we can presume that the foreign body was not ingested and the child can be discharged home with safety net advice. This can be found on the Wessex Healthier Together website by searching for foreign body (swallowed).
If the foreign body is radiolucent e.g. wooden toothpick, a referral to a surgical specialty should be made regardless of X-ray findings. In most cases this will be paediatric surgery (<16 years) or adult endoscopy (16 or 17 years). However, if the child has symptoms of upper oesophageal or airway obstruction such as drooling, gagging or stridor, an ENT referral is more appropriate.
Irrespective of the type of foreign body ingested, symptoms are suggestive of complications such as obstruction, perforation or erosion. These patients should be referred to the relevant specialty, even if the foreign body is not visualised on X-ray. Stridor, drooling, gagging and dysphagia are suggestive of upper oesophageal obstruction requiring ENT referral. Vomiting and abdominal pain are suggestive of a more distal obstruction requiring paediatric surgery or adult endoscopy input.
A foreign body visualised above the level of the clavicles suggests upper oesophageal obstruction and requires referral to ENT. A patient with a foreign body visualised below the level of the clavicles should be referred to paediatric surgery (if aged under 16 years) or adult endoscopy (16 or 17 years). However, in some regional centres ENT are able to remove foreign bodies further down the oesophagus, so consider discussing with your local ENT service as well as paediatric surgery.
If the FB is not seen on chest X-ray consider whether it could be more proximal or distal to what has been imaged and obtain a soft tissue neck and/or abdominal X-ray. Even if the FB is radiolucent and unlikely to be visualised on X-ray (e.g. a wooden toothpick), a chest X-ray is useful to exclude complications such as pneumomediastinum and pneumoperitoneum.
If the suspected foreign body is a radiopaque material, cannot be visualised on X-ray and the child is well, we can presume that the foreign body was not ingested and the child can be discharged home with safety net advice. This can be found on the Wessex Healthier Together website by searching for foreign body (swallowed).
If the foreign body is radiolucent e.g. wooden toothpick, a referral to a surgical specialty should be made regardless of X-ray findings. In most cases this will be paediatric surgery (<16 years) or adult endoscopy (16 or 17 years). However, if the child has symptoms of upper oesophageal or airway obstruction such as drooling, gagging or stridor, an ENT referral is more appropriate.
Irrespective of the type of foreign body ingested, symptoms are suggestive of complications such as obstruction, perforation or erosion. These patients should be referred to the relevant specialty, even if the foreign body is not visualised on X-ray. Stridor, drooling, gagging and dysphagia are suggestive of upper oesophageal obstruction requiring ENT referral. Vomiting and abdominal pain are suggestive of a more distal obstruction requiring paediatric surgery or adult endoscopy input.
Button Batteries
Ingestion of button batteries can cause serious harm and should be treated as an emergency even if the child is asymptomatic. A senior clinician should be informed of the child on triage, chest and abdominal X-rays organised and urgent referral to the appropriate specialty without delay.
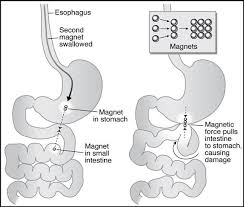
Button batteries can cause harm via several mechanisms (1); Direct pressure, Chemical damage and electrical damage, with animal models demonstrating necrosis within 15 minutes of Ingestion (2). If the battery is lodged in the oesophagus this is particularly concerning, as fistulation into the trachea or major blood vessels can occur.
Button batteries lodged in the oesophagus or airway should be removed within 2 hours of presentation to minimise mucosal damage. This should take place even if the child is asymptomatic or has eaten recently. Co-ingestion of a button battery and magnet also requires emergency removal regardless of where it is in the GI system.
Animal studies have found that early administration of honey or sucralfate solution can reduce the depth and severity of injury from button battery ingestion (3). Therefore, if XR indicates a button battery is lodged in the oesophagus, the child is > 12 months of age and presents within 12 hours of ingestion, administer:
Button batteries can cause harm via several mechanisms (1); Direct pressure, Chemical damage and electrical damage, with animal models demonstrating necrosis within 15 minutes of Ingestion (2). If the battery is lodged in the oesophagus this is particularly concerning, as fistulation into the trachea or major blood vessels can occur.
Button batteries lodged in the oesophagus or airway should be removed within 2 hours of presentation to minimise mucosal damage. This should take place even if the child is asymptomatic or has eaten recently. Co-ingestion of a button battery and magnet also requires emergency removal regardless of where it is in the GI system.
Animal studies have found that early administration of honey or sucralfate solution can reduce the depth and severity of injury from button battery ingestion (3). Therefore, if XR indicates a button battery is lodged in the oesophagus, the child is > 12 months of age and presents within 12 hours of ingestion, administer:
Sucralfate solution 1g orally every 10 minutes for 3 doses.
Do not delay endoscopic removal to complete this treatment. The patient should otherwise be kept nil by mouth whilst awaiting endoscopy.
If the battery has passed into the stomach it will usually transit spontaneously through the rest of the GI tract. Provided the child is asymptomatic a conservative approach can be taken with a repeat abdominal X-ray on day 4. The child should still be referred to paediatric surgery who will confirm that this management is appropriate.
Other Types of Batteries
These are less dangerous than button batteries but may still leak and cause erosion. Obtain a chest X-ray and refer to the appropriate specialty for advice.
If the battery has passed into the stomach it will usually transit spontaneously through the rest of the GI tract. Provided the child is asymptomatic a conservative approach can be taken with a repeat abdominal X-ray on day 4. The child should still be referred to paediatric surgery who will confirm that this management is appropriate.
Other Types of Batteries
These are less dangerous than button batteries but may still leak and cause erosion. Obtain a chest X-ray and refer to the appropriate specialty for advice.
Magnets
|
Rare-earth magnets such as Neodymium magnets are up to 15 times more powerful than traditional magnets. They are inexpensive and readily available, often used in children’s toys, manufacturing and adult toys marketed as stress relievers. Since they are small and brightly coloured they are easily ingested by young children. There have also been case reports of older children using magnets as fake tongue and cheek piercings, leading to accidental ingestion.
A rise in these presentations led to a National Patient Safety Alert (4) and release of an RCEM Best Practice Guideline (5) in May 2021. |
|
|
Ingesting >1 magnet or co-ingesting a magnet and a metal object should be treated as an emergency even if the child is asymptomatic. This is because they can be attracted to each other within the body, trapping pieces of bowel and causing perforation or obstruction. Weaker “ordinary” magnets can also cause serious harm and should be managed in the same way.
|
|
Management
Obtain a chest and abdominal X-ray (with the child lying down, ideally prone) to assess the number and position of magnets ingested. Symptomatic patients, those who have ingested >1 magnet or co-ingested a magnet and another metal foreign body should be discussed with paediatric surgery. Intestinal injury can occur within 8 hours of ingestion, thus symptomatic or unwell patients require urgent surgical review.
Single Magnet Ingestion
Ingestion of a single rare-earth magnet is unlikely to cause harm. In this scenario first confirm that there is only one foreign body by obtaining a lateral abdominal X-ray. On a single X-ray view multiple magnets may appear as a single foreign body due to their alignment.
If a single magnet ingestion is confirmed and all of the criteria in Box 1 are met, a “watch and wait” approach can be taken. The patient can be discharged home with a plan to return to the Emergency Department in 6-12 hours for a repeat abdominal X-ray. The child should be discharged with safety net advice which includes returning to the Emergency Department straight away should they develop symptoms, and advised to remove external metal objects such as metallic buttons or belt buckles. A safety net advice sheet can be found on the Wessex Healthier Together website by searching for foreign body (swallowed).
Obtain a chest and abdominal X-ray (with the child lying down, ideally prone) to assess the number and position of magnets ingested. Symptomatic patients, those who have ingested >1 magnet or co-ingested a magnet and another metal foreign body should be discussed with paediatric surgery. Intestinal injury can occur within 8 hours of ingestion, thus symptomatic or unwell patients require urgent surgical review.
Single Magnet Ingestion
Ingestion of a single rare-earth magnet is unlikely to cause harm. In this scenario first confirm that there is only one foreign body by obtaining a lateral abdominal X-ray. On a single X-ray view multiple magnets may appear as a single foreign body due to their alignment.
If a single magnet ingestion is confirmed and all of the criteria in Box 1 are met, a “watch and wait” approach can be taken. The patient can be discharged home with a plan to return to the Emergency Department in 6-12 hours for a repeat abdominal X-ray. The child should be discharged with safety net advice which includes returning to the Emergency Department straight away should they develop symptoms, and advised to remove external metal objects such as metallic buttons or belt buckles. A safety net advice sheet can be found on the Wessex Healthier Together website by searching for foreign body (swallowed).
Criteria for Discharging Single Magnet Ingestions with Planned Follow Up
- Single magnet ingestion
- Asymptomatic
- Accidental ingestion
- No co-morbidities
- Tolerating oral intake
- Presents within 24hr of ingestion
- Care-giver able to provide close observation
- Easily able to return to the hospital in event of deterioration
Repeat imaging is necessary to confirm that the magnet is progressing through the GI tract and beyond the small bowel. Repeat imaging should be performed with the child in the same position (lying down, ideally prone) and interpreted by a radiologist.
If the magnet is failing to progress through the GI tract on serial imaging, the child should be referred to paediatric surgery. If the magnet is progressing through the GI tract beyond the small bowel and the child remains asymptomatic, they can be discharged with safety net advice. This can be found on the Wessex Healthier Together website by searching for foreign body (swallowed).
Management of Asymptomatic, Non-Hazardous Ingestions
Some children and parents will not know what type of foreign body has been ingested. In this situation it is safest to assume it is a “hazardous object”.
Non-Metallic Objects
e.g. small plastic toy
Children who have swallowed a non-metallic, non-hazardous object, have no symptoms and are able to eat and drink can be discharged with safety net advice. This can be found on the Wessex Healthier Together website by searching for foreign body (swallowed).
Consider the need for a psychiatric assessment and mental health follow up.
Consider whether there are any safeguarding concerns and raise as per local policy if applicable.
Metallic Objects
e.g. coin, jewellery
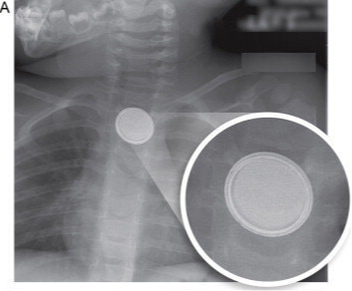
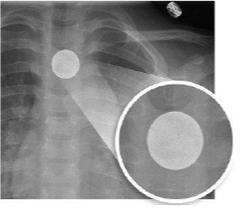
Particular care should be taken to ensure “coins” are not hazardous button batteries – take a careful history and if in any doubt obtain PA and lateral X-rays looking for the “halo” sign. If still unsure discuss with a senior clinician and consider referring to a specialist.
e.g. small plastic toy
Children who have swallowed a non-metallic, non-hazardous object, have no symptoms and are able to eat and drink can be discharged with safety net advice. This can be found on the Wessex Healthier Together website by searching for foreign body (swallowed).
Consider the need for a psychiatric assessment and mental health follow up.
Consider whether there are any safeguarding concerns and raise as per local policy if applicable.
Metallic Objects
e.g. coin, jewellery
Particular care should be taken to ensure “coins” are not hazardous button batteries – take a careful history and if in any doubt obtain PA and lateral X-rays looking for the “halo” sign. If still unsure discuss with a senior clinician and consider referring to a specialist.
|
Left - a button battery with double ring or halo sign. On lateral view you may see a central bulge.
Right - a coin with homogenous appearance. Reproduced from Jatana (6) |
|
|
Metallic objects can be detected by both Hand Held Metal Detectors (HHMD) and X-rays. A HHMD is quicker to use and does not expose the child to radiation, therefore it should be the first-line investigation. A systematic review comparing the accuracy of HHMDs against X-ray, found the HHMD had an overall sensitivity of 99.4% when detecting the presence of an ingested coin and 99.8% in locating the coin (7). See below for guidance on how to use a hand held metal detector.
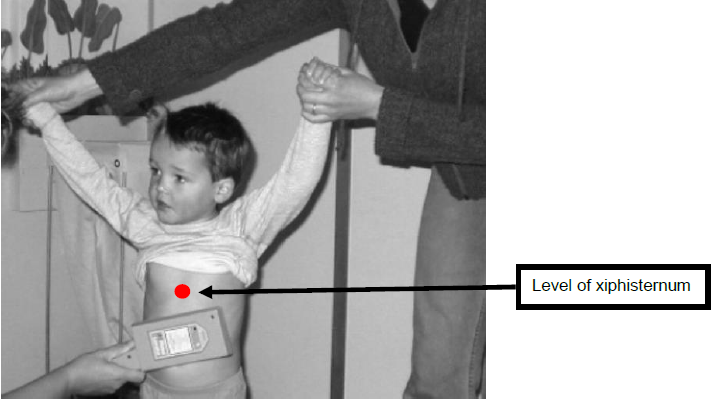
- Beep above xiphisternum: Obtain chest X-ray
- Ambiguous result: Obtain chest X-ray
- Beep below xiphisternum: Discharge with safety net advice
- No beep: Discharge with safety net advice
If there is no beep or the beep is below the xiphisternum, the child can be discharged home with safety net advice. This can be found on the Wessex Healthier Together website by searching for foreign body (swallowed).
Consider the need for a psychiatric assessment and mental health follow up.
Consider whether there are any safeguarding concerns and refer as per local policy if applicable.
If the beep is above the xiphisternum or the result is ambiguous, obtain a chest X-ray +/- neck X-ray.
- No FB identified on X-ray: discharge home with safety net advice as detailed above.
- FB above the clavicles: refer to ENT
- FB between the clavicles and diaphragm and child <16 years old: refer to paediatric surgery.
- FB between clavicles and diaphragm and child 16 or 17 years old: refer to adult endoscopist.
- FB below the diaphragm: discharge home with safety net advice as detailed above.
How to use a Hand Held Metal Detector (HHMD)
When using a HHMD first confirm it is working by testing against a known metal object such as the metal rail of a trolley. The presence of a metal object should result in a visual and auditory response such as a beep and flashing red light.
When scanning, the child should be standing upright or be supported upright by their parent/carer. All jewellery and metal clothing such as zips should be removed, and scanning should take place away from metal objects such as the trolley or metal wall fixtures.
Hold the HHMD 2-4cm away from the child and scan from the nose down to the level of the pubic symphysis in the midline. Repeat the process left and right of the midline to cover three vertical lines down the child anteriorly, then repeat all three lines posteriorly.
If there is a beep determine whether the object is above or below the diaphragm, using the surface anatomy of the xiphisternum as the level of the diaphragm. The significance of this is that an object above the diaphragm is likely to be lodged and require intervention to be removed, whereas an object below the diaphragm is likely to pass spontaneously.
Caution should be taken with morbidly obese children and those with known metal implants. If in doubt about the accuracy of the HHMD obtain a chest X-ray.
References
- Jatana KR, Rhoades K, Milkovich S, Jacobs IN (2016) Basic mechanism of button battery ingestion injuries and novel mitigation strategies after diagnosis and removal. Laryngoscope 127(6):1276-1282
- Tanaka J, Yamashita M, Yamashita M, Kajigaya H (1998) Esophageal electrochemical burns due to button type lithium batteries in dogs. Vet Hum Toxicol 40(4):193–196
- Anfang RR et al (2019) pH-neutralizing Esophageal Irrigations as a Novel Mitigation Strategy for Button Battery Injury Laryngoscope, 129:49-57
- Urgent Assessment/Treatment following Ingestion of “Super-Strong” Magnets, 2021, National Patient Safety Agency, Accessed June 2021
<http://www.england.nhs.uk/wp-content/uploads/2021/05/NaPSA-Alert-Magnets-FINAL-v5.pdf> - Ingestion of Super Strong Magnets in Children, 2021, RCEM, Accessed June 2021
<http://www.rcem.ac.uk/docs/RCEM_BPC_Ingestion_of_Super_Strong_Magnets_in_Children_170521.pdf> - Jatana K. Button Battery Injuries in Children: A Growing Risk. Everything Matters in Patient Care. Nationwide Children’s Hospital, Columbus, OH; 2013
- J B Lee, S Ahmad, C P Gale (2005) Detection of coins ingested by children using a handheld metal detector: a systematic review. Emerg Med J; 22:839–844.
|
Document Version:
1.6 Lead Authors: D. James, Paed Emergency Medicine Consultant, UHS R. Broomfield, Paed Emergency Medicine Consultant, UHS M. Stanton, Paediatric Surgical Consultant, UHS K. Lines, Emergency Medicine Trainee |
Approving Network:
Wessex Paediatric Emergency Medicine Clinical Network Date of Approval: March 2022 Review Due: March 2025 |
PIER Contact |
|