Antenatally Detected Uropathy:
Investigations and Management Guideline
Investigations and Management Guideline
Flowcharts
Multicystic Dysplastic Kidney
|
Renal Pelvis Dilatation
|
Duplex System
|
Introduction
The following is a modified aid for the management of antenatally detected urinary tract anomalies. It has been completed following a multidisciplinary meeting, involving representatives from the departments of genetics, fetal medicine, obstetric ultrasonography, neonatology, radiology and nephro-urology. Where possible it has relied on published evidence but when such evidence was not available the aid incorporates the clinical experience and opinions of the experienced clinicians involved. Many of the approaches are already practised by other units in this country.
Dr Arvind Nagra, Dr Matthew Harmer (Consultant Paediatric Nephrologists) and Mr Ewan Brownlee (Consultant Paediatric Urologist), are the Lead Postnatal Clinicians in this area and will coordinate antenatal counselling and postnatal management. The other clinicians listed are also happy to provide advice, antenatal counselling or take over the management of patients when appropriate.
Within UHS
Postnatally it is the responsibility of the person performing the first medical examination (or admitting person if baby comes to NNU) to initiate investigation and referral if appropriate, and to organise follow up and action of early scan results (those required within 2 weeks). Please discuss your plan with the neonatal consultant responsible for the postnatal ward.
Please also request any scans or investigations required within 6 weeks of birth (usually MCDK or hydronephrosis). Inform the neonatal renal lead consultant of baby’s birth, contact details for mother, and plan by email. He/ she will chase the results and action them. Babies who require follow up but do not meet criteria for tertiary renal services will be referred to the lead general paediatrician at SGH.
Their contact details are listed at the end of this guideline.
The following is a modified aid for the management of antenatally detected urinary tract anomalies. It has been completed following a multidisciplinary meeting, involving representatives from the departments of genetics, fetal medicine, obstetric ultrasonography, neonatology, radiology and nephro-urology. Where possible it has relied on published evidence but when such evidence was not available the aid incorporates the clinical experience and opinions of the experienced clinicians involved. Many of the approaches are already practised by other units in this country.
Dr Arvind Nagra, Dr Matthew Harmer (Consultant Paediatric Nephrologists) and Mr Ewan Brownlee (Consultant Paediatric Urologist), are the Lead Postnatal Clinicians in this area and will coordinate antenatal counselling and postnatal management. The other clinicians listed are also happy to provide advice, antenatal counselling or take over the management of patients when appropriate.
Within UHS
Postnatally it is the responsibility of the person performing the first medical examination (or admitting person if baby comes to NNU) to initiate investigation and referral if appropriate, and to organise follow up and action of early scan results (those required within 2 weeks). Please discuss your plan with the neonatal consultant responsible for the postnatal ward.
Please also request any scans or investigations required within 6 weeks of birth (usually MCDK or hydronephrosis). Inform the neonatal renal lead consultant of baby’s birth, contact details for mother, and plan by email. He/ she will chase the results and action them. Babies who require follow up but do not meet criteria for tertiary renal services will be referred to the lead general paediatrician at SGH.
Their contact details are listed at the end of this guideline.
Scope and Purpose
These guidelines apply to babies diagnosed with a congenital abnormality of the urinary tract antenatally.
These guidelines apply to babies diagnosed with a congenital abnormality of the urinary tract antenatally.
General Principles
Isolated dilatation of renal pelvis (no calyceal/ureteric dilatation) with an anteroposterior (ap) diameter < 10mm
Calyceal/ureteric dilatation irrespective of renal pelvis diameter (RPD)
All bladder outlet obstructions & ureteroceles require early surgical intervention.
Multicystic dysplastic kidneys
Renal Agenesis
Fusion or migration abnormalities (cross fused renal ectopia, horseshoe kidney, ectopic kidney)
All following should be referred to urology specialist postnatally
Micturating cystourethrogram
Isolated dilatation of renal pelvis (no calyceal/ureteric dilatation) with an anteroposterior (ap) diameter < 10mm
- During last trimester virtually always benign.
- No prophylactic antibiotics but give parents information leaflet re UTI.
- No postnatal investigation.
Calyceal/ureteric dilatation irrespective of renal pelvis diameter (RPD)
- May be significant
- Refer to specific guidance in relevant sections
All bladder outlet obstructions & ureteroceles require early surgical intervention.
- Refer immediately to urologist.
Multicystic dysplastic kidneys
- If contralateral kidney normal, benign condition
- Most will involute spontaneously.
Renal Agenesis
- Unilateral renal agenesis should be managed as per Simple MCDK if the solitary kidney has a normal appearance
- It should be managed as per complicated MCDK if the single kidney has abnormalities
Fusion or migration abnormalities (cross fused renal ectopia, horseshoe kidney, ectopic kidney)
- The postnatal management is dictate by the presence or absence of hydronephrosis
All following should be referred to urology specialist postnatally
- Bilateral RPD 15mm with no reflux
- Non-Refluxing megaureters
- Dilatation of a solitary kidney
- Dilatation in any moiety of a duplex kidney
- Unilateral RPD 30mm
- Progressive increase in dilatation on 2 consecutive scans or cortical thinning
- Differential function < 40%
- Development of symptoms such as pain/UTI
Micturating cystourethrogram
- Do immediately if bladder outlet obstruction suspected, with gentamicin cover
- Otherwise avoid till 6/12 old unless symptomatic and/or suspecting obstructive pathology when MCUG followed by Diuretic Renography will be indicated
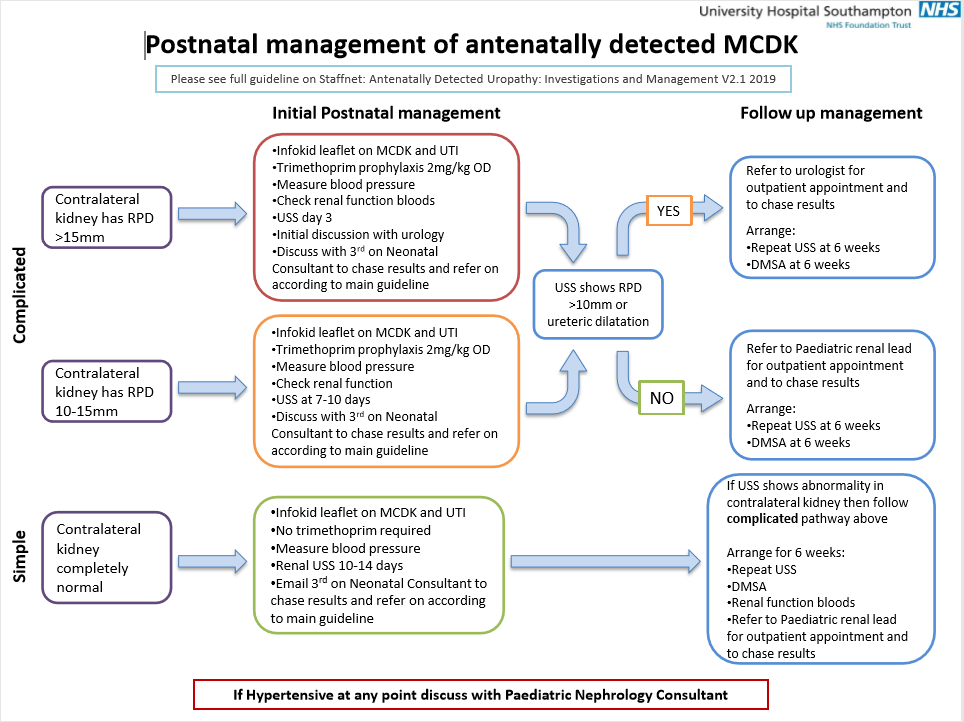
Multicystic Dysplastic Kidney
Antenatal
Postnatal
Simple (provide same management for unilateral renal agensis with normal single kidney)
Indications for referral/nephrectomy
Complicated – Give InfoKid leaflet on MCDK to parents
Dilatation of contralateral >15mm antero-posterior RPD
Dilatation of contralateral > 10mm <15mm/ureteric/calyceal dilation
Antenatal
- 20/40 scan, refer Fetal Medicine or obstetrician
- Refer to Dr Nagra antenatally
- If contralateral kidney normal, repeat scan @ 32/40.
Postnatal
- Simple: The contralateral side is completely normal
- Complicated: There is an abnormality of the contralateral side
Simple (provide same management for unilateral renal agensis with normal single kidney)
- At Birth - Give InfoKid leaflet to parents (https://www.infokid.org.uk/MCDK)
- Measure blood pressure. No need for prophylactic antibiotics
- Arrange first postnatal renal ultrasound scan at 10-14 days old
- Follow-up with neonatal renal lead consultant
- Discuss results with renal specialist (at UHS) if any abnormality in non-cystic/single kidney or hypertensive.
- At 6 weeks old
- Repeat US Scan (not for unilateral agenesis). Discuss with nephro-urology team if any abnormality in contralateral non-cystic kidney or increase in size of MCDK
- DMSA (if there is any function in presumed MCDK it is NOT MCDK: refer to urologist) + baseline renal bloods
- Outpatient follow-up with imaging results + measure BP
- If well, no treatment and see at one year old but warn parents and GP of risks of UTI (give leaflet).
- At one year
- Repeat US Scan – ensure non-cystic kidney normal with evidence of hypertrophy of contralateral kidney
- Measure BP + check albumin:creatinine ratio
- Long-term follow-up
- Repeat renal US Scan aged 2 yrs, 5 years and 10 years looking for evidence of contralateral renal hypertrophy. If no hypertrophy for referral to nephrologists.
- Yearly BP and urine dipstick – lifelong
- Formal GFR after 2 years of age. If unable to do formally then use estimated GFR using calculation (height (cm) x 40/creatinine)
- If good contralateral renal hypertrophy, normal GFR, normotensive and no proteinuria - discharge to GP for life-long yearly BP and proteinuria assessment (enclose sex-appropriate BP centile chart) after 10 year US Scan with a written follow-up plan for the patient and GP and the reason they need long term follow-up. Include InfoKid leaflet on MCDK.
Indications for referral/nephrectomy
- Increasing size/ significant solid component.
- Hypertension / symptoms.
- Albuminuria
- Renal tract dilatation
Complicated – Give InfoKid leaflet on MCDK to parents
Dilatation of contralateral >15mm antero-posterior RPD
- Prophylactic antibiotics (Trimethoprim 2mg/kg/day (max 100mg) ON)/refer to neonatal renal lead consultant / exclude obstruction
- US Scan day 3 (earlier if reduced amniotic fluid volumes) and d/w paediatric urologist for further advice
- Check renal function
- Check BP
- 6 weeks: MAG3 Renogram + Repeat US Scan
Dilatation of contralateral > 10mm <15mm/ureteric/calyceal dilation
- Prophylactic antibiotics (Trimethoprim 2mg/kg/day (max 100mg) ON)/refer to neonatal renal lead consultant
- Check renal function.
- Check BP
- USS at 7-10 days
- If RPD >10mm, ureteric dilatation or ureteric dilatation persists d/w paediatric urology team
- 6 weeks; MAG3 Renogram + Repeat US Scan
- If no obstruction repeat US scan at 3 month, 6 months and 12 months
- If repeat US Scan shows increasing dilatation d/w paediatric urologist/nephrologist.
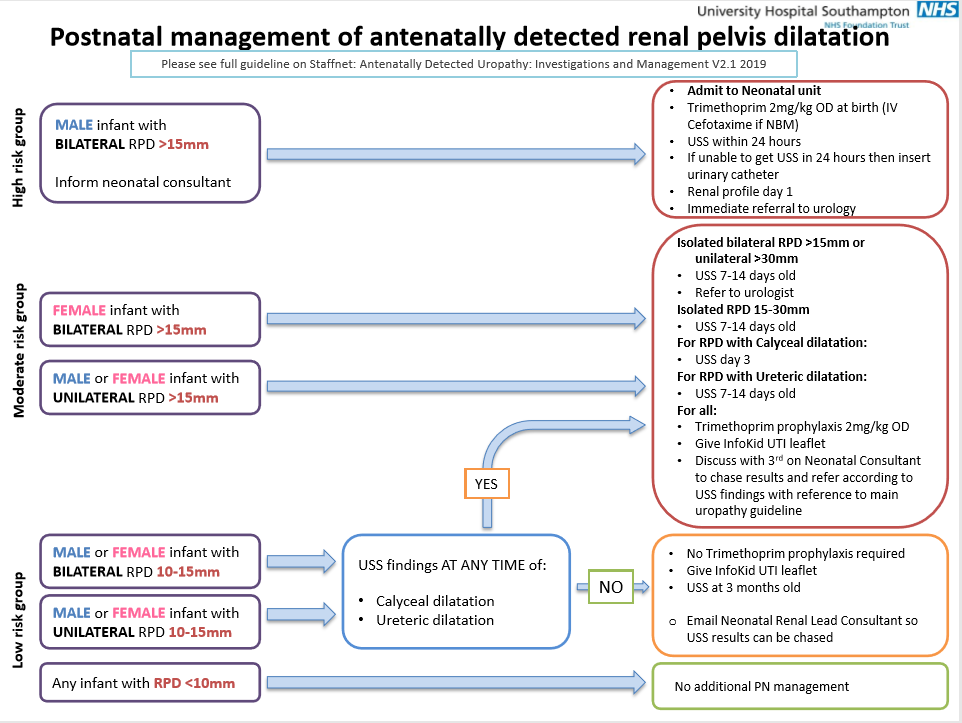
Renal Pelvis Dilatation
Note renal pelvic diameter should be measured anteroposteriorly on transverse plane.
Isolated Renal Pelvis Dilatation >7mm <10mm AP DIAM
Antenatal
Isolated Renal Pelvis Dilatation >10mm <15mm AP DIAM
Antenatal
At Birth
Renal Pelvis of Any Diameter and Calyceal Dilatation
Antenatal
At Birth
Renal pelvis of any diameter + ureteric dilatation (see below for bladder outlet obstruction)
At Birth
To exclude obstruction
Any renal pelvis dilatation > 15mm AP DIAM
Antenatal
At Birth
6 weeks
12 months
Note renal pelvic diameter should be measured anteroposteriorly on transverse plane.
Isolated Renal Pelvis Dilatation >7mm <10mm AP DIAM
Antenatal
- Detected 20/40
- One further scan only @ 32/40, if still <10mm antenatally discharge with information leaflet on UTI (https://www.infokid.org.uk/urinary-tract-infection-uti)
Isolated Renal Pelvis Dilatation >10mm <15mm AP DIAM
Antenatal
- Detected 20/40. Refer Fetal Medicine. Give appropriate InfoKid information leaflet (https://www.infokid.org.uk/antenatal-hydronephrosis)
- One further scan only @ 32/40 in main department. If <10mm discharge and no need for postnatal investigations. If still >10 and < 15mm investigate postnatally.
At Birth
- No prophylactic antibiotics but provide information leaflet on UTI on discharge
- Refer to neonatal renal lead consultant
- US Scan @ 3/12 old, if still < 15mm discharge with a further information leaflet on UTI (https://www.infokid.org.uk/urinary-tract-infection-uti)
Renal Pelvis of Any Diameter and Calyceal Dilatation
Antenatal
- Detected 20/40; refer to Fetal Medicine
- One further scan only @ 32/40, if still same investigate postnatally
At Birth
- Antibiotic prophylaxis - Trimethoprim 2mg/kg/day (max 100mg) ON.
- Provide information leaflet on UTI (https://www.infokid.org.uk/urinary-tract-infection-uti)
- Refer to neonatal renal lead consultant
- Renal US Scan – day 3.
- If AP diameter > 15mm treat as 'Any renal pelvis dilatation >15mm AP DIAM'
- If AP < 15 mm and calyceal dilatation persists repeat US Scan @ 6/52
- If still < 15mm and calyceal dilation persists but not increased- repeat US Scan at 3/12
- If still < 15mm but calyceal dilation increased or thought significant by radiologist- refer to neonatal renal lead consultant to exclude reflux or obstruction
Renal pelvis of any diameter + ureteric dilatation (see below for bladder outlet obstruction)
At Birth
- Prophylactic antibiotics - Trimethoprim 2mg/kg/day (max 100mg) ON
- Provide information leaflet on UTI (https://www.infokid.org.uk/urinary-tract-infection-uti)
- US Scan @ 7-14 days old, if ureter still dilated, d/w paediatric urologist .re need for MCUG if male.
To exclude obstruction
- MAG3 renogram @ 6 weeks + Repeat renal US Scan
Any renal pelvis dilatation > 15mm AP DIAM
Antenatal
- If unilateral refer Fetal Medicine, multiple scans not necessary
- If bilateral in male consider bladder outlet obstruction and scan regularly
- Refer for antenatal counselling with Dr Arvind Nagra if bilateral or if > 30mm unilateral
At Birth
- Start prophylactic antibiotics - Trimethoprim 2mg/kg/day (max 100mg) ON.
- If unilateral male/female, US Scan @ 7 - 14 days old
- If bilateral male, admit to Neonatal unit, US Scan within 1st 24 hours, check bloods, assess bladder. If unable to obtain scan within 24 hours catheterise pending results of MCUG. Strict fluid input and output chart- may get post-obstructive diuresis. Correct any fluid/electrolyte disturbance
- Any suspicion of bladder outlet obstruction, do MCUG within 48 hours under gentamicin cover (2.5 mgs/kg)
- If unilateral and AP Diam > 30mm or bilateral >15mm refer to urologist
- If unilateral and AP Diam > 15mm - < 30mm, refer to neonatal renal lead consultant
6 weeks
- US Scan + MAG3 renogram
- If function < 40% refer urologist
- If function >40%, US Scan at 3, 6 &12 months; Repeat MAG3 at 12 months
- If function reduces or increasing RPD or pain/UTI refer to paediatric urologist.
12 months
- If remains stable but dilated, yearly US Scan for 5 years
- If stable at end of 5 years, repeat MAG3
- If function stable and no obstruction repeat ultrasound after 2 years. Consider discharging if asymptomatic and appearances stable. Give advice to remain vigilant for UTI and loin pain. If this develops then will need re-imaging.
Bladder Outlet Obstruction
Suspect if there is:
Antenatal
At Birth
Obstruction confirmed
Suspect if there is:
- Bilateral hydroureteronephrosis/hydroureteronephrosis in a solitary kidney
- Incomplete bladder emptying
- Thick walled bladder
- Dilated posterior urethra
- Urinary ascites
- Unilateral urinoma
- Unilateral hydronephrosis + oligohydramnios in a male infant.
Antenatal
- Refer to Fetal Medicine
- Repeat scans regularly to monitor dilatation/renal echogenicity/liquor volumes
- Refer to Dr Arvind Nagra.
At Birth
- Prophylactic antibiotics - Trimethoprim 2mg/kg/day (max 100mg) ON.
- US Scan within 1st 24 hours
- If obstruction still suspected MCUG (iv gentamicin 2.5 mg/kg)
- If unable to obtain scan within 24 hours catheterise pending results of MCUG
- Strict fluid input and output chart – may get post-obstructive diuresis. Correct any fluid/electrolyte disturbance
Obstruction confirmed
- Leave catheter in situ on free drainage
- Refer immediately to urologist
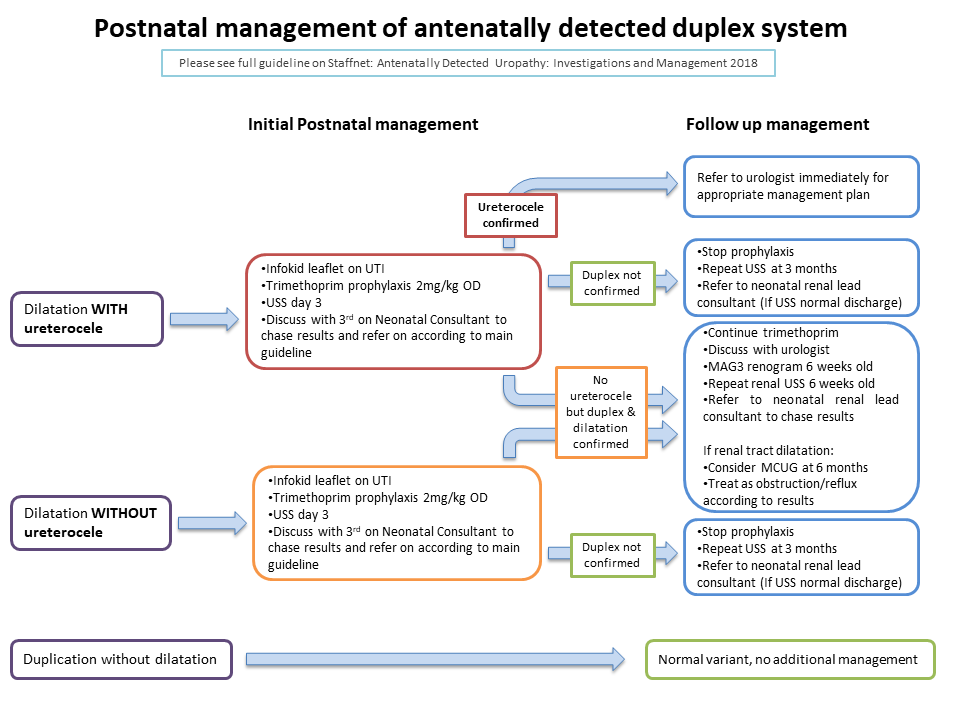
Duplex Systems
Duplication without dilatation is a variation of anatomy and not pathological. It requires no further investigation or treatment.
With dilatation & ureterocele
Antenatal
At Birth
Ureterocele confirmed
No ureterocele but Duplex confirmed
Duplex not confirmed
Dilatation but without ureterocele
When a duplex is suspected and there is dilatation of the upper moiety and there is no ureterocele
Duplication without dilatation is a variation of anatomy and not pathological. It requires no further investigation or treatment.
With dilatation & ureterocele
Antenatal
- Refer to Fetal Medicine
- Repeat US Scan @ 32/40, no need for serial scans
- Refer to Dr Arvind Nagra
- If utererocele suspected, baby can be delivered in a local hospital.
At Birth
- Prophylactic antibiotics - Trimethoprim 2mg/kg/day (max 100mg) ON.
- Refer neonatal renal lead consultant
- US Scan @ 72 hours old
Ureterocele confirmed
- Refer to urologist immediately to decide the need for urgent surgical intervention
No ureterocele but Duplex confirmed
- Continue prophylaxis (Trimethoprim 2mg/kg/day (max 100mg) ON)
- MAG3 renogram @ 6 weeks old + Repeat renal USS
- Consider MCUG @ 6 months if renal tract dilatation
- Treat as obstruction/reflux depending on results.
Duplex not confirmed
- Stop prophylaxis
- Repeat US Scan @ 3 months. If normal, discharge
Dilatation but without ureterocele
When a duplex is suspected and there is dilatation of the upper moiety and there is no ureterocele
- Start antibiotic prophylaxis - Trimethoprim 2mg/kg/day (max 100mg) ON.
- Refer to neonatal renal lead consultant
- US Scan @ 3 days. If confirmed d/w paediatric urologist as there is still a risk of obstruction or ureteric ectopia both of which can develop major complications such as pyoureteronephrosis.
Contact Details
Consultant Paediatric Nephrologists
Consultant Paediatric Urologists
UHS Neonatal Renal Lead
Consultant Paediatric Nephrologists
- Dr Arvind Nagra
- Dr Rodney Gilbert
- Dr Shuman Haq
- Dr Matthew Harmer
- Contact via secretary - 023 8120 6254/5222
Consultant Paediatric Urologists
- Mr Stephen Griffin
- Mr Sengamalai (Mano) Manoharan
- Mr Ewen Brownlee
- Contact via secretary - 023 8120 8464/5222
UHS Neonatal Renal Lead
- Can be contacted via secretary - 023 8120 4920
Governance
Roles and Responsibilities
This policy applies to staff employed or contracted by UHS NHS Foundation Trust and to other clinicians in the Wessex region referring to Southampton as the tertiary centre. Every member of staff has a personal responsibility to ensure they comply with this document. It is the responsibility of departmental managers, consultants, team leads and education leads to ensure that their staff are aware of this policy.
Implementation
The guideline will be displayed on the Staffnet, and sent to the relevant Care Group clinical teams. The team leaders will be expected to cascade to all relevant groups.
Process for Monitoring Compliance/Effectiveness
The purpose of monitoring is to provide assurance that the agreed approach is being followed – this ensures we get things right for patients, use resources well and protect our reputation. Our monitoring will therefore be proportionate, achievable and deal with specifics that can be assessed or measured.
Arrangements for Review of the Policy
Every 3 years or if there is a change to national guidance.
Roles and Responsibilities
This policy applies to staff employed or contracted by UHS NHS Foundation Trust and to other clinicians in the Wessex region referring to Southampton as the tertiary centre. Every member of staff has a personal responsibility to ensure they comply with this document. It is the responsibility of departmental managers, consultants, team leads and education leads to ensure that their staff are aware of this policy.
Implementation
The guideline will be displayed on the Staffnet, and sent to the relevant Care Group clinical teams. The team leaders will be expected to cascade to all relevant groups.
Process for Monitoring Compliance/Effectiveness
The purpose of monitoring is to provide assurance that the agreed approach is being followed – this ensures we get things right for patients, use resources well and protect our reputation. Our monitoring will therefore be proportionate, achievable and deal with specifics that can be assessed or measured.
Arrangements for Review of the Policy
Every 3 years or if there is a change to national guidance.
References
- Bouzada et al 2004. Diagnostic accuracy of fetal renal pelvis anteroposterior diameter as a predictor of uropathy: a prospective study. Ultrasound Obstet Gynecol 24: 745-9
- Coelho et al 2007. Outcome of isolated antenatal hydronephrosis: a prospective cohort study. Pediatr. Nephrol 22:1727-1734
- Cohen-OverbeeK et al 2005. Mild renal pyelectasis in the second trimester: determination of cut-off levels for postnatal referral. Ultrasound Obstet Gynecol 25: 378-83
- Damen-Elias et al 2005. Mild pyelectasis diagnosed by prenatal ultrasound is not a predictor of urinary tract morbidity in childhood. Prenatal Diagnosis 25: 1239-47.
- Lee et al 2006. Antenatal hydronephrosis as a predictor of postnatal outcome: a metaanalysis. Paediatrics 118 (2): 586-593
- Wollenberg et al 2005. Outcome of fetal renal pelvic dilatation diagnosed during the third trimester. Ultrasound Obstet Gynecol 25: 483-8.
|
Document Version:
5.0 Lead Author: Dr Arvind Nagra, Consultant Paediatric Nephrologist Dr Karen Brackley, Consultant Obstetrician Mr Henrik Steinbrecher, Consultant Paediatric Urologist Dr Kelly Brown, Consultant Neonatologist |
Approving Network:
Wessex Paediatric Nephro-Urology Network Date of Approval: 03/2022 Review Date: 03/2025 |
PIER Contact |
|