Kawasaki Disease:
Diagnosis, Management, Follow-up & Referral
Diagnosis, Management, Follow-up & Referral
Flowcharts
Flow Chart 1: Kawasaki Disease Algorithm
(Click to expand)
(Click to expand)
Flow Chart 2: Evaluation of Suspected Kawasaki Disease or Incomplete Kawasaki Disease
(Click to expand)
(Click to expand)
Flowchart 3: Echocardiography Timeline and Follow-up for Kawasaki Disease
(Click to expand)
(Click to expand)
Introduction
This guideline applies to all paediatric patients (under 16 years)
Kawasaki disease is the second most common systemic vasculitis in childhood and is the commonest cause of acquired heart disease in the UK through a predilection for the coronary arteries. Kawasaki disease is:-
Kawasaki disease is the second most common systemic vasculitis in childhood and is the commonest cause of acquired heart disease in the UK through a predilection for the coronary arteries. Kawasaki disease is:-
- most commonly seen in children from 6 months to 5 years (peak 8 to 24 months)
- more common in winter and spring,
- more common in boys
- more common in East Asian populations.
Scope & Purpose
This guidance has been developed to aid the diagnosis and management of children with possible Kawasaki disease in Wessex using available skills and network links.
Early recognition and appropriate treatment may reduce the risk of coronary involvement and subsequent complications from up to 25% to nearer 3%. Diagnosis is reliant on clinical features and may be difficult as there is no diagnostic test and there may be considerable overlap with other conditions at initial presentation (see section 3). Some children are at risk of IVIG resistance and rapid evolution of coronary artery aneurysms (see section 6). Therefore, discussion with Southampton ID or rheumatology teams is recommended if risk factors are present for IVIG resistance or the patient is unresponsive to the 1st dose of intravenous immunoglobulin (IVIG), to decide if adjuvant immunosuppressive therapy, such as steroids, is required in addition to IVIG.
Early recognition and appropriate treatment may reduce the risk of coronary involvement and subsequent complications from up to 25% to nearer 3%. Diagnosis is reliant on clinical features and may be difficult as there is no diagnostic test and there may be considerable overlap with other conditions at initial presentation (see section 3). Some children are at risk of IVIG resistance and rapid evolution of coronary artery aneurysms (see section 6). Therefore, discussion with Southampton ID or rheumatology teams is recommended if risk factors are present for IVIG resistance or the patient is unresponsive to the 1st dose of intravenous immunoglobulin (IVIG), to decide if adjuvant immunosuppressive therapy, such as steroids, is required in addition to IVIG.
Definitions & Diagnosis
Classical Kawasaki Disease
Diagnostic criteria for classical Kawasaki disease
Table 1: Classical Features of Kawasaki Disease
Diagnostic criteria for classical Kawasaki disease
- Fever for ≥ 5 days + ≥ 4/5 clinical features
- Fever <5 days + all 5 clinical features + persistently elevated inflammatory markers without alternative cause. Treatment of such cases at less than 5 days of fever should be discussed with UHS ID or rheumatology teams.
Table 1: Classical Features of Kawasaki Disease
Clinical Feature |
Unusual Characteristics/Notes |
Fever for ≥ 5 days |
|
Cervical Lymphadenopathy |
|
Oral Changes |
|
Rash |
|
Conjunctival Injection |
|
Extremity Changes |
|
Figure 1
from Son MBSRP. Kawasaki disease.In: Petty RELRMLCBWLR editor. Textbook of Pediatric Rheumatology, Vol 7 Philadelphia, PA: Elsevier; (2016).p. 467-83
from Son MBSRP. Kawasaki disease.In: Petty RELRMLCBWLR editor. Textbook of Pediatric Rheumatology, Vol 7 Philadelphia, PA: Elsevier; (2016).p. 467-83
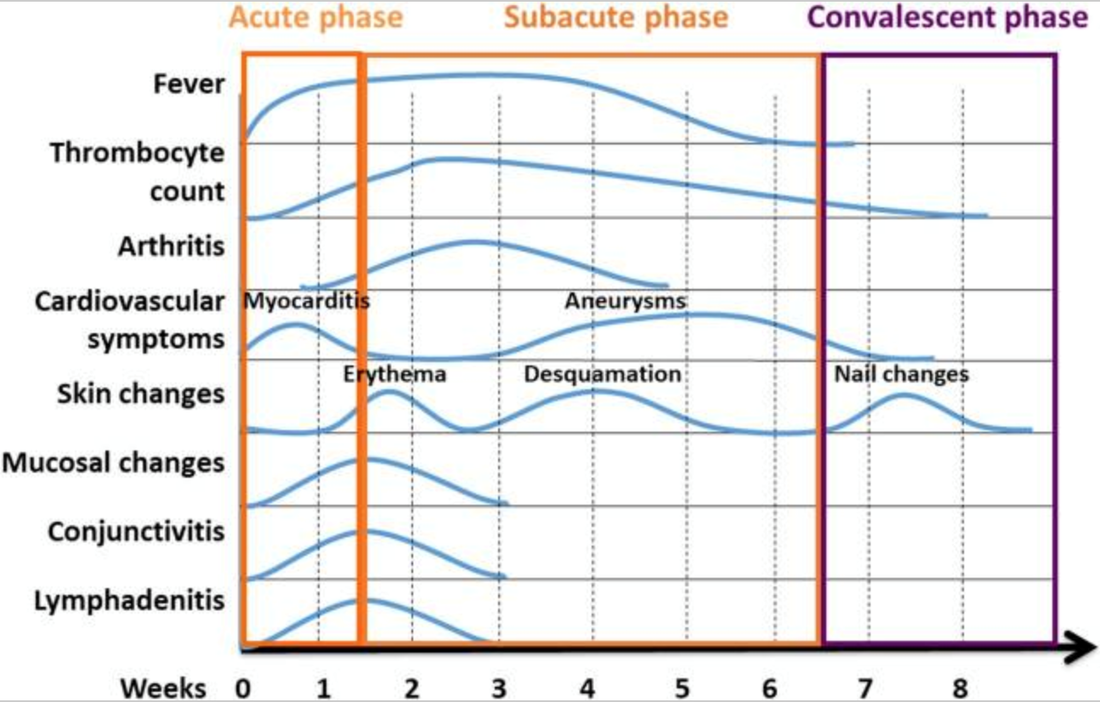
Kawasaki disease constitute a systemic inflammatory disorder with an acute, subacute and convalescent phase. The clinical features of Kawasaki disease vary over the course of the disease and not all are present at the same time. Often rashes which developed after commencing antibiotic can be mistaken for allergic drug reaction. Careful review of history and assessment of each clinical features are crucial to avoid missing the diagnosis.
Other clinical features and complications
Other features may support the diagnosis and relate to the complications of the condition. For example:
Non-Cardiac Complications and Associated Clinical Features
Other clinical features and complications
Other features may support the diagnosis and relate to the complications of the condition. For example:
Non-Cardiac Complications and Associated Clinical Features
Aseptic Meningitis |
|
Gallbladder hydrops (10%) Diarrhoea (20%) Hepatitis Pancreatitis |
|
Myositis Arthralgia and Arthritis (30%) |
|
Urethritis or Meatitis |
|
Aneurysmal arteries |
|
Pro-inflammatory state |
|
Atypical/incomplete Kawasaki disease
If patients do not meet the classic criteria they may either have atypical/incomplete Kawasaki disease or an alternative diagnosis (see further information). Atypical Kawasaki disease is more common in infants and in children over 7 years and these groups have a high risk of coronary artery complications if not treated. In up to 90% the absent cardinal feature is cervical lymphadenopathy, and in up to 50% the rash may not be present. In infant under 6 months, prolonged fever and irritability may be the only features of Kawasaki disease.
Incomplete Kawasaki disease should be suspected and laboratory investigations performed in:
Supportive lab investigations and findings on early echocardiography are aids to making a diagnosis. Features increasing the likelihood of incomplete Kawasaki disease that would benefit from IVIG include any of the following:
Atypical Kawasaki disease should also be suspected in the following group of patients:
Definition of prolonged fever:
Discussion with the UHS ID/rheumatology team is highly recommended in all cases of incomplete Kawasaki disease or suspected Kawasaki disease to avoid delay in diagnosis and treatment and to exclude other differential diagnosis. Patient who do not meet the criteria for classical and atypical Kawasaki disease but continue to have persistent fever should be re-evaluated and discussed with the UHS ID/rheumatology team. Be wary that the presence of concurrent infection does not exclude the diagnosis of Kawasaki disease as up to 33% children with Kawasaki disease have a concurrent infection. In order to treat Kawasaki disease effectively it is important to reach a diagnosis and commence treatment before the 10th day of the illness.
Note: It is suggested that all children presenting with suspected Kawasaki disease are started on ceftriaxone 80mg/kg on admission. Resolution of fever following commencement of IV antibiotics makes a diagnosis of KD extremely unlikely.
If patients do not meet the classic criteria they may either have atypical/incomplete Kawasaki disease or an alternative diagnosis (see further information). Atypical Kawasaki disease is more common in infants and in children over 7 years and these groups have a high risk of coronary artery complications if not treated. In up to 90% the absent cardinal feature is cervical lymphadenopathy, and in up to 50% the rash may not be present. In infant under 6 months, prolonged fever and irritability may be the only features of Kawasaki disease.
Incomplete Kawasaki disease should be suspected and laboratory investigations performed in:
- Infants under 6 months with prolonged unexplained fever for ≥ 7 days even in the absence of clinical feature of Kawasaki disease
- Children of any age with unexplained fever for ≥ 5 days and with only 2-3 clinical features (see Table 1).
Supportive lab investigations and findings on early echocardiography are aids to making a diagnosis. Features increasing the likelihood of incomplete Kawasaki disease that would benefit from IVIG include any of the following:
- CRP ≥30mg/L or ESR ≥40mm/hr AND 3 abnormal laboratory findings
- Abnormal echocardiography
- Infant <6 months of age with fever for ≥ 7 days even without supportive clinical or laboratory findings without any alternative diagnosis.
Atypical Kawasaki disease should also be suspected in the following group of patients:
- Infant with prolonged fever and unexplained aseptic meningitis
- Infants or children with prolonged fever and unexplained or culture-negative shock
- Infants or children with prolonged fever and cervical lympahadenitis unresponsive to antibiotic therapy
- Infants or children with prolonged fever and retropharyngeal or parapharyngeal phlegmon unresponsive to antibiotic therapy
Definition of prolonged fever:
- Fever ≥7 days in infant <6 months
- Fever ≥5 days in those > 6 months
Discussion with the UHS ID/rheumatology team is highly recommended in all cases of incomplete Kawasaki disease or suspected Kawasaki disease to avoid delay in diagnosis and treatment and to exclude other differential diagnosis. Patient who do not meet the criteria for classical and atypical Kawasaki disease but continue to have persistent fever should be re-evaluated and discussed with the UHS ID/rheumatology team. Be wary that the presence of concurrent infection does not exclude the diagnosis of Kawasaki disease as up to 33% children with Kawasaki disease have a concurrent infection. In order to treat Kawasaki disease effectively it is important to reach a diagnosis and commence treatment before the 10th day of the illness.
Note: It is suggested that all children presenting with suspected Kawasaki disease are started on ceftriaxone 80mg/kg on admission. Resolution of fever following commencement of IV antibiotics makes a diagnosis of KD extremely unlikely.
Macrophage activation syndrome (MAS)
MAS is a known complication of KD. It is a secondary form of haemophagocytic lymphohistiocytosis (HLH).
Features of MAS include:
Consider this diagnosis in refractory KD and discuss with UHS rheumatology regarding management (usually IV prednisolone +/- anakinra)
MAS is a known complication of KD. It is a secondary form of haemophagocytic lymphohistiocytosis (HLH).
Features of MAS include:
- Persistent high fever and high CRP
- High (or rising) Ferritin (>1000). Daily counts helpful in sick children
- Cytopenias (at least 2 lineages) or falling counts (so falling Hb/Platelets/WBC likely significant even if absolute numbers remain in normal range)
- Low ESR and fibrinogen
- High Triglycerides and LFTs
Consider this diagnosis in refractory KD and discuss with UHS rheumatology regarding management (usually IV prednisolone +/- anakinra)
Differential diagnosis
Many childhood illnesses may be confused with Kawasaki disease on initial presentation. These include: -
However, with careful attention to the evolution of the clinical picture, results of investigations, and response to 24 - 48 of antibiotic therapy the diagnosis is likely to be clarified.
Many childhood illnesses may be confused with Kawasaki disease on initial presentation. These include: -
- Group A streptococcal infection +/- toxin mediated disease
- Staphylococcus aureus infection +/- toxin medicated disease
- Viral infections – Adenovirus, enterovirus, measles, EBV
- Stevens-Johnson syndrome
- Systemic juvenile idiopathic arthritis
- Measles
However, with careful attention to the evolution of the clinical picture, results of investigations, and response to 24 - 48 of antibiotic therapy the diagnosis is likely to be clarified.
Investigations
First line investigations during acute illness
There are no diagnostic tests for Kawasaki disease and the diagnosis relies on clinical criteria, supported by evidence of inflammation, whilst ruling out other differential diagnoses. There are some characteristic laboratory findings in Kawasaki disease which may help in atypical cases. Other investigations may be helpful in clarifying an alternative diagnosis where there is uncertainty.
There are no diagnostic tests for Kawasaki disease and the diagnosis relies on clinical criteria, supported by evidence of inflammation, whilst ruling out other differential diagnoses. There are some characteristic laboratory findings in Kawasaki disease which may help in atypical cases. Other investigations may be helpful in clarifying an alternative diagnosis where there is uncertainty.
Investigation |
Expected Findings |
Additional Notes |
Hb |
|
|
WCC |
|
|
Platelets |
|
|
CRP |
|
|
ESR |
|
|
Ferritin |
|
|
LFTs & U&Es |
|
|
Blood Culture |
|
|
ASOT Anti-DNase B Bacterial Throat Swab for respiratory viruses including enterovirus |
|
|
Urine dip and micro |
|
|
Second line investigations during acute illness
If no response to IV antibiotics by 24- 48 hours, remains febrile and no alternative diagnosis reached, suggest proceeding to 2nd line investigations. Recommend discussion with UHS ID or rheumatology team in such cases in order to review need for urgent echocardiogram.
If no response to IV antibiotics by 24- 48 hours, remains febrile and no alternative diagnosis reached, suggest proceeding to 2nd line investigations. Recommend discussion with UHS ID or rheumatology team in such cases in order to review need for urgent echocardiogram.
Investigation |
Additional Notes |
C3/C4 ANA / ANCA Ferritin |
|
EBV serology CMV serology Parvovirus serology Measles PCR |
|
Mycoplasma titres |
|
Stool for enterovirus |
|
Abdominal USS |
|
CXR |
|
LDH, VMAs etc |
|
Treatment
Immunoglobulin (IVIG)
Following diagnosis patients with Kawasaki disease should be commenced on treatment with intravenous immunoglobulin and aspirin.
Treatment with intravenous immunoglobulin within the first 10 days of the onset of the illness reduces the complications, mortality and morbidity of Kawasaki disease. There may still be limited benefit of treatment from 10 to 60 days if there are ongoing active signs of inflammation, persistent unexplained fever or coronary artery changes evident on echocardiogram.
Immunoglobulin should be prescribed on an intravenous fluid chart as 'Normal Immunoglobulin for Intravenous Use at a dose of 2 g/kg given over 12 hours'. If there are features of heart failure (disproportionate tachycardia, gallop rhythm, liver enlargement, breathlessness) then discuss the rate of administration with the duty consultant due to the risk of cardiac decompensation.
If risk factors for IVIG resistance (age <1 year, plts <100, liver derangement - ALT>100), to discuss with UHS ID or rheumatology team regarding need for adjuvant immunosuppression (oral prednisolone 2mg/kg for 3 days followed by wean over 2 weeks) in addition to first dose of IVIG and role of urgent echocardiogram. If shock/haemodynamic instability, consider adding methylprednisolone with first dose of IVIG.
Immunoglobulin side effects include chills, malaise, fever, haemolytic anaemia, aseptic meningitis and rarely anaphylaxis.
Administration issues with immunoglobulin
Aspirin
Although aspirin is normally contraindicated in children under 16 years due to the risk of Reye’s syndrome it is recommended in children with Kawasaki disease. Aspirin treatment is started at high dose for anti-inflammatory effects, and reduced to lower dose for anti-platelet effects (see below for further information). The low dose aspirin is continued until the coronary arteries have been shown to appear normal.
High dose aspirin should initially be prescribed on the drug chart (and discharge medication sheet) at a dose of 7.5 to 12.5 mg/kg four times a day, equivalent to a total daily dose of 30-50 mg/kg (maximum dose 4g/day). This dose is administered by dispersing 75 mg tablets in 5 mls of water (equivalent to 15 mg/ml) and drawing up the appropriate volume. (Note that 300 mg tablets are also available but their use should be avoided to prevent confusion).
When to stop high dose aspirin and switch to maintenance low dose aspirin:
Low dose aspirin should be prescribed on the discharge medication sheet at a dose of 2 to 5 mg/kg once daily, with instruction to change from high dose to this lower dose once fever subsided for 24 hours and CRP is improving. This dose is administered by dispersing 75 mg tablets in 5 mls of water (equivalent to 15 mg/ml) and drawing up the appropriate volume. (Note that 300 mg tablets are also available but their use should be avoided to prevent confusion). Ensure that the family and GP are aware that repeat prescriptions will be needed. Low dose aspirin should continue until at least the 6-8 week echocardiogram.
Warfarin
Patients with giant coronary artery aneurysms with or without stenosis are at the highest risk for coronary thrombosis due to abnormal flow conditions. In addition, the presence of chronic thrombus in the aneurysms can amplify the thrombotic cascade. Therefore, warfarin should be commenced for patients with giant coronary artery aneurysms with initial full heparinisation to prevent thrombosis. Aim for an INR range of 2-2.5.
Expected response to therapy
80-90% respond to above treatment within 36 hours with a settling of temperature. If symptoms persist at 48 hours or recur within 2 weeks of initial treatment and there is no alternative diagnosis identified then discuss with UHS paediatric ID or rheumatology teams regarding differential diagnoses, the role of an urgent echocardiogram and whether 2nd line treatment should include adjuvant steroids along with a second dose of IVIG.
MMR/Varicella vaccination
Administration of IVIG can interfere with the immune response to parenteral live vaccines if given concomitantly with or shortly before or after the vaccine. In accordance to the Green book, it is recommended that MMR and Varicella vaccination are deferred for 3 month post IVIG but immune response likely to be higher when deferred for 9 month post IVIG. No repeat dose of vaccination is needed if the vaccine was administrated 14 days or more prior to IVIG.
Following diagnosis patients with Kawasaki disease should be commenced on treatment with intravenous immunoglobulin and aspirin.
Treatment with intravenous immunoglobulin within the first 10 days of the onset of the illness reduces the complications, mortality and morbidity of Kawasaki disease. There may still be limited benefit of treatment from 10 to 60 days if there are ongoing active signs of inflammation, persistent unexplained fever or coronary artery changes evident on echocardiogram.
Immunoglobulin should be prescribed on an intravenous fluid chart as 'Normal Immunoglobulin for Intravenous Use at a dose of 2 g/kg given over 12 hours'. If there are features of heart failure (disproportionate tachycardia, gallop rhythm, liver enlargement, breathlessness) then discuss the rate of administration with the duty consultant due to the risk of cardiac decompensation.
If risk factors for IVIG resistance (age <1 year, plts <100, liver derangement - ALT>100), to discuss with UHS ID or rheumatology team regarding need for adjuvant immunosuppression (oral prednisolone 2mg/kg for 3 days followed by wean over 2 weeks) in addition to first dose of IVIG and role of urgent echocardiogram. If shock/haemodynamic instability, consider adding methylprednisolone with first dose of IVIG.
Immunoglobulin side effects include chills, malaise, fever, haemolytic anaemia, aseptic meningitis and rarely anaphylaxis.
Administration issues with immunoglobulin
- Consent forms are not required.
- Record batch number and product name in notes.
- Different manufacturers / products have specific instructions on infusion rates – see the package insert.
- Please note that this is a “red” indication for immunoglobulin and the necessary local immunoglobulin request paperwork will need to be completed
Aspirin
Although aspirin is normally contraindicated in children under 16 years due to the risk of Reye’s syndrome it is recommended in children with Kawasaki disease. Aspirin treatment is started at high dose for anti-inflammatory effects, and reduced to lower dose for anti-platelet effects (see below for further information). The low dose aspirin is continued until the coronary arteries have been shown to appear normal.
High dose aspirin should initially be prescribed on the drug chart (and discharge medication sheet) at a dose of 7.5 to 12.5 mg/kg four times a day, equivalent to a total daily dose of 30-50 mg/kg (maximum dose 4g/day). This dose is administered by dispersing 75 mg tablets in 5 mls of water (equivalent to 15 mg/ml) and drawing up the appropriate volume. (Note that 300 mg tablets are also available but their use should be avoided to prevent confusion).
When to stop high dose aspirin and switch to maintenance low dose aspirin:
- Resolution of fever for 24 hours AND
- CRP/inflammatory markers trending downward (does not have to be normal value)
Low dose aspirin should be prescribed on the discharge medication sheet at a dose of 2 to 5 mg/kg once daily, with instruction to change from high dose to this lower dose once fever subsided for 24 hours and CRP is improving. This dose is administered by dispersing 75 mg tablets in 5 mls of water (equivalent to 15 mg/ml) and drawing up the appropriate volume. (Note that 300 mg tablets are also available but their use should be avoided to prevent confusion). Ensure that the family and GP are aware that repeat prescriptions will be needed. Low dose aspirin should continue until at least the 6-8 week echocardiogram.
Warfarin
Patients with giant coronary artery aneurysms with or without stenosis are at the highest risk for coronary thrombosis due to abnormal flow conditions. In addition, the presence of chronic thrombus in the aneurysms can amplify the thrombotic cascade. Therefore, warfarin should be commenced for patients with giant coronary artery aneurysms with initial full heparinisation to prevent thrombosis. Aim for an INR range of 2-2.5.
Expected response to therapy
80-90% respond to above treatment within 36 hours with a settling of temperature. If symptoms persist at 48 hours or recur within 2 weeks of initial treatment and there is no alternative diagnosis identified then discuss with UHS paediatric ID or rheumatology teams regarding differential diagnoses, the role of an urgent echocardiogram and whether 2nd line treatment should include adjuvant steroids along with a second dose of IVIG.
MMR/Varicella vaccination
Administration of IVIG can interfere with the immune response to parenteral live vaccines if given concomitantly with or shortly before or after the vaccine. In accordance to the Green book, it is recommended that MMR and Varicella vaccination are deferred for 3 month post IVIG but immune response likely to be higher when deferred for 9 month post IVIG. No repeat dose of vaccination is needed if the vaccine was administrated 14 days or more prior to IVIG.
Cardiac Involvement in Kawasaki Disease
Cardiac involvement in Kawasaki disease
Transthoracic echocardiography has high sensitivity and specificity for identifying cardiac involvement in Kawasaki disease. Coronary artery abnormality is the commonest complication of untreated Kawasaki disease but other cardiac involvement includes:
However, timing of echocardiography should not delay the initiation of IVIG.
If Kawasaki disease is strongly suspected in patients who do not fulfill all the clinical criteria for diagnosis of Kawasaki disease such as those with suspected incomplete Kawasaki disease, an urgent echocardiography can be diagnostic. Presence of coronary artery abnormality on echocardiography is diagnostic of incomplete Kawasaki disease.
A baseline ECG should be obtained in all patients treated with Kawasaki disease.
Echocardiography assessment
Patients with diagnosis of Kawasaki disease who have received IV immunoglobulin need follow-up echocardiography and ECG on at least 2 occasions, at 2-3 weeks and 6-8 weeks after diagnosis (see Follow-up arrangement). Coronary artery dilatation can be difficult to assess in the acute phase of Kawasaki disease. Therefore, all patients with the diagnosis of Kawasaki disease must be referred to the paediatric cardiologists at UHS for an echocardiographic assessment but do not delay administration of IVIG whilst waiting for echocardiogram.
Children with Kawasaki disease are usually very irritable and may not tolerate echocardiography. Sedation with chloral hydrate or midazolam (see local sedation protocol) may be required for detailed echocardiographic studies. In a distressed child, imaging of the coronary arteries is given priority to sequential segmental imaging. Coronary arteries are assessed using the highest frequency probe and multiple views before concluding the presence or absence of coronary artery involvement. Coronary artery aneurysms may increase in size over the first 4-6 weeks after onset of illness. Approximately 50-75% of aneurysms regress to normal lumen diameter within the first 2 years and further regression is unlikely thereafter. The likelihood of the aneurysm regressing to normal lumen diameter is strongly related to its maximum diameter. Giant aneurysms are least likely to regress. Younger children, those at a more distal location or fusiform shape are more likely to regress.
Features of abnormal coronary arteries in Kawasaki disease are:
In order of highest to lowest frequency, common sites of coronary aneurysms are:
Coronary artery measurements should be taken from the inner edge to inner edge of the vessel wall, avoiding the orifices and points of branching which may have normal focal dilatation. The internal lumen diameter is then normalized for body surface area as a Z-score. Various body surface area (BSA) and Z-score formulae are available. Medcon in UHS uses Haycock formula for BSA. Studies have shown that CA Z scores <3 correlate well between formulae but can vary significantly at larger CA dimensions potentially affecting the decision of anticoagulant. It is important that the same Z score and BSA formula are used at the initial CA measurement and subsequent follow up echocardiogram especially in the first 6 weeks of illness.
Transthoracic echocardiography has high sensitivity and specificity for identifying cardiac involvement in Kawasaki disease. Coronary artery abnormality is the commonest complication of untreated Kawasaki disease but other cardiac involvement includes:
- Valvar regurgitation
- Pericardial effusion suggesting pericarditis
- Papillary muscle brightness and impaired left ventricular systolic function suggesting myocarditis
- Aortic root dilatation (usually mild)
However, timing of echocardiography should not delay the initiation of IVIG.
If Kawasaki disease is strongly suspected in patients who do not fulfill all the clinical criteria for diagnosis of Kawasaki disease such as those with suspected incomplete Kawasaki disease, an urgent echocardiography can be diagnostic. Presence of coronary artery abnormality on echocardiography is diagnostic of incomplete Kawasaki disease.
A baseline ECG should be obtained in all patients treated with Kawasaki disease.
Echocardiography assessment
Patients with diagnosis of Kawasaki disease who have received IV immunoglobulin need follow-up echocardiography and ECG on at least 2 occasions, at 2-3 weeks and 6-8 weeks after diagnosis (see Follow-up arrangement). Coronary artery dilatation can be difficult to assess in the acute phase of Kawasaki disease. Therefore, all patients with the diagnosis of Kawasaki disease must be referred to the paediatric cardiologists at UHS for an echocardiographic assessment but do not delay administration of IVIG whilst waiting for echocardiogram.
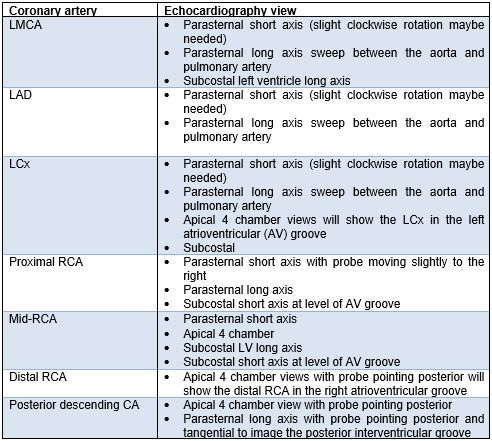
Children with Kawasaki disease are usually very irritable and may not tolerate echocardiography. Sedation with chloral hydrate or midazolam (see local sedation protocol) may be required for detailed echocardiographic studies. In a distressed child, imaging of the coronary arteries is given priority to sequential segmental imaging. Coronary arteries are assessed using the highest frequency probe and multiple views before concluding the presence or absence of coronary artery involvement. Coronary artery aneurysms may increase in size over the first 4-6 weeks after onset of illness. Approximately 50-75% of aneurysms regress to normal lumen diameter within the first 2 years and further regression is unlikely thereafter. The likelihood of the aneurysm regressing to normal lumen diameter is strongly related to its maximum diameter. Giant aneurysms are least likely to regress. Younger children, those at a more distal location or fusiform shape are more likely to regress.
Features of abnormal coronary arteries in Kawasaki disease are:
- Perivascular brightness or lack of tapering of the distal coronary artery may also suggest coronary artery involvement in Kawasaki disease
- Dilatation (z score >2, < 2.5)
- Aneurysm (their shape and size can evolve over time. See below for further classification)
- Saccular
- Fusiform
- Ectatic (diffusely dilated without a segmental aneurysm)
In order of highest to lowest frequency, common sites of coronary aneurysms are:
- Proximal left anterior descending (LAD)
- Proximal right coronary artery (RCA)
- Left main coronary artery (LMCA)
- Left circumflex (LCx)
- Distal RCA
- Junction between the RCA and posterior descending coronary artery
Coronary artery measurements should be taken from the inner edge to inner edge of the vessel wall, avoiding the orifices and points of branching which may have normal focal dilatation. The internal lumen diameter is then normalized for body surface area as a Z-score. Various body surface area (BSA) and Z-score formulae are available. Medcon in UHS uses Haycock formula for BSA. Studies have shown that CA Z scores <3 correlate well between formulae but can vary significantly at larger CA dimensions potentially affecting the decision of anticoagulant. It is important that the same Z score and BSA formula are used at the initial CA measurement and subsequent follow up echocardiogram especially in the first 6 weeks of illness.
Classification of Coronary Artery |
Size of Coronary Artery Abnormality |
Dilated CA |
Z score >2 to <2.5 |
Small aneurysm |
Z score ≥ 2.5 to < 5 |
Medium aneurysm |
Z score ≥5 to <10 and absolute diameter <8mm |
Giant aneurysm |
Z score ≥ 10 or absolute diameter of ≥8mm |
In addition to the coronary arteries, left ventricular (LV) function should also be routinely assessed in patients with Kawasaki disease. LV systolic function should be assessed using a combination of techniques i.e M-mode, 2-D approach and Simpson biplane technique and not only rely on visual assessment. These techniques allow quantification of fractional shortening (FS), fractional area change (FAC) and ejection fraction (EF) which are useful in long-term follow-up.
Discharge
The following criteria are a guide prior to discharge:
- 36 hours or more has elapsed since the completion of intravenous immunoglobulin
- Fever has settled (less than 37.5 for at least 24 hours)
- Aspirin is tolerated orally
- The child’s family understand the regime of aspirin treatment
- The child’s family understand the need to obtain repeat prescription of aspirin from GP
- The discharge letter includes advice that live vaccines (MMR or varicella) should be deferred for at least 3 months following immunoglobulin therapy.
Follow up
Kawasaki disease-related vasculopathy is characterized by myointimal proliferation with or without layering of thrombus which may lead to progressive coronary artery stenosis. Patients with coronary artery aneurysm carry a lifelong increase risk of coronary artery thrombosis and stenosis which may results in myocardial ischaemia, infarction and sudden death. Therefore, children with Kawasaki disease with coronary artery involvement should be followed-up.
Follow-up recommendations:
Normal coronary artery and no other cardiac involvement
Coronary artery dilatation (Z score >2.0, <2.5)
Small coronary artery aneurysm (Z score ≥ 2.5, <5)
Medium size coronary artery aneurysm (Z score ≥ 5 to <10 and absolute diameter <8mm)
Giant coronary artery aneurysm (Z score ≥ 10mm or absolute diameter ≥8mm)
Follow-up recommendations:
Normal coronary artery and no other cardiac involvement
- For non-urgent echo and ECG at 2 weeks after onset of illness and repeat echo in 6 weeks
- Follow up in the local joint cardiac clinic or paediatric cardiology clinic in University Hospital Southampton
- Discontinue maintenance dose of aspirin at 6 weeks if echo remains normal
- Review again in 1 year and if continue to have normal coronary artery, discharge from clinic
- Offer healthy lifestyle advice to minimize cardiovascular risk factors- No smoking, moderate alcohol consumption and regular exercise.
Coronary artery dilatation (Z score >2.0, <2.5)
- Repeat echo and ECG at 2 weeks and 6 weeks after diagnosis
- Continue on aspirin until dilatation resolved
- For resolved, transient coronary artery dilatation, subsequent follow up beyond a year at the discretion of the consultant paediatric cardiologist.
- Can be discharged or
- Follow up
- For persistent dilatation, continue to follow up and reassess every 2-5 years
- Other investigations to consider:
- Stress imaging
- Calcium CT score
- Exercise tolerance test (ETT) if clinically indicated i.e chest pain or breathlessness
- Advice to inform paediatric cardiologist urgently if develop chest pain
- Healthy lifestyle advice to reduce cardiovascular risk factors (see above)
Small coronary artery aneurysm (Z score ≥ 2.5, <5)
- Repeat echo and ECG at 2 weeks and 6 weeks after diagnosis
- Subsequent echo at 6 monthly to 1 yearly interval (longer if resolved aneurysm)
- Continue on aspirin until aneurysm resolved
- Consider imaging of the coronary artery with CT/MRI or angiogram
- Other investigations to consider:
- Stress imaging
- CT calcium score
- Exercise tolerance test (ETT) if clinically indicated i.e chest pain or breathlessness
- Advice to inform paediatric cardiologist urgently if develop chest pain
- Healthy lifestyle advice to reduce cardiovascular risk factors (see above)
- Refer to interventional cardiologist for lifelong follow-up
Medium size coronary artery aneurysm (Z score ≥ 5 to <10 and absolute diameter <8mm)
- Repeat echo and ECG at 2 weeks and 6 weeks after diagnosis
- Subsequent echo at 6 monthly to 1 yearly interval (longer if resolved aneurysm)
- Continue on aspirin until aneurysm resolved
- Consider imaging of the coronary artery with CT/MRI or angiogram
- Other investigations to consider:
- Stress imaging
- CT calcium score
- Exercise tolerance test (ETT) if clinically indicated i.e chest pain or breathlessness
- Advice to inform paediatric cardiologist urgently if develop chest pain
- Healthy lifestyle advice to reduce cardiovascular risk factors (see above)
- Refer to interventional cardiologist for lifelong follow-up
Giant coronary artery aneurysm (Z score ≥ 10mm or absolute diameter ≥8mm)
- Lifelong maintenance dose of aspirin
- Add Warfarin (Target INR 2-2.5). Heparin should be started to prevent thrombosis.
- Weekly echocardiography to monitor progression of aneurysm size or thrombus formation
- Frequency of further follow-up is at the discretion of consultant paediatric cardiologist
- Imaging of the coronary artery using CT or MRI to monitor progression of and assessment for coronary artery stenosis
- Other investigations to consider:
- Coronary artery angiography (wait at least 6 months from acute presentation)
- Stress imaging
- ETT if clinically indicated (see above)
- Exercise restriction advice (avoid high intensity exercise)
- Advice to inform paediatric cardiologist urgently if develop chest pain
- Healthy lifestyle advice to reduce cardiovascular risk factors
- Refer to interventional cardiologist for lifelong follow-up
Implementation and Monitoring
This guideline will be displayed on the PIER network website, accessible to all paediatrician working within the Wessex region.
Audit results will be circulated and presented at the multidisciplinary audit meetings, identified in the monitoring table. Any areas of non compliance or gaps in assurance that arise from the monitoring of this guideline will result in an action plan detailing recommendations and proposals to address areas of non compliance and/or embed learning. Monitoring of these plans will be coordinated by the group/committee identified in the monitoring table. The resulting actions will be reviewed or followed up at the subsequent multidisciplinary audit meeting(s).
Audit results will be circulated and presented at the multidisciplinary audit meetings, identified in the monitoring table. Any areas of non compliance or gaps in assurance that arise from the monitoring of this guideline will result in an action plan detailing recommendations and proposals to address areas of non compliance and/or embed learning. Monitoring of these plans will be coordinated by the group/committee identified in the monitoring table. The resulting actions will be reviewed or followed up at the subsequent multidisciplinary audit meeting(s).
References
- McCrindle B, Rowley A, Newburger J, et al. Diagnosis, treatment and long-term management of Kawasaki disease: A scientific statement for health professionals from the American heart association. Circulation (2017); 135:e927-e999
- Ryu K, Yu J J, Jun H O, et al. A comparative study of established z score models for coronary artery diameters in 181 healthy Korean children. Korean J Pediatr (2017);60 (11):373-378
- Ronai C, Hamaoka-Okamoto A, Baker A L, et al. Coronary artery aneurysm measurement and Z score variability in Kawasaki disease. J Am Soc Echocardiogr (2016);29(2): 150-157
- Dietz SM, Tacke CE, Kuipers IM, et al. Cardiovascular imaging in children and adults following Kawasaki disease. Insights Imaging. (2015);6:697-705
- BNF for children 2014-2015. BMJ Group. ISBN 978 0 85369 847
- Manlhiot C, Niedra E, McCrindle B. Long-term management of Kawasaki disease: Implications for the adult patient. Pediatrics and neonatology (2013);54:12-21
- Eleftheriou D, et al. Arch Dis Child 2014;99:74–83. doi:10.1136/archdischild-2012-302841
- Manlhiot C, Millar K, Golding F, McCrindle B. Improved classification of coronary artery abnormalities based only on coronary artery z-scores after Kawasaki disease. Pediatr Cardiol (2010);31:242-249
- IK Maconochie. Kawasaki disease. Arch. Dis. Child. Ed. Pract. Ed. (2004); 89: 3-8.
- Baumer JH, Love S, Gupta A, Haines L, Maconochie IK, Dua JS. Salicylate for the treatment of Kawasaki disease in children. Cochrane Database of Systematic Reviews (2006), Issue 4.
- AF Freeman, ST Shulman. Kawasaki Disease: Summary of the American Heart Association guidelines. Am Fam Physician (2006);74:1141-8, 1149-50
- LE Wood, RMR Tulloh. Kawasaki disease in children. Heart (2009) 95: 787-792.
- JH Baumer. Kawasaki disease: What to do with incomplete cases. Arch Dis Child Educ Pract Ed (2005); 90: ep102 – ep104.
- Benseler SM, McCrindle BW, Silverman ED, et al. Infections and Kawasaki disease: implications for coronary artery outcome. Pediatrics (2005);116:e760
- Oates-Whitehead RM, Baumer JH, Haines L, Love S, Maconochie IK, Gupta A, Roman K, Dua JS, Flynn I. Intravenous immunoglobulin for the treatment of Kawasaki disease in children. Cochrane Database of Systematic Reviews (2003), Issue 4.
- P A Brogan, A Bose, D Burgner, D Shingadia, R Tulloh, C Michie, N Klein, R Booy, M Levin and M J Dillon. Kawasaki disease: an evidence based approach to diagnosis, treatment, and proposals for future research. Arch. Dis. Child. (2002);86;286-290
- Kato H, Sugimura T, Akagi T, et al. Long-term consequences of Kawasaki disease. A 10-21 year long follow-up study of 594patients. Circulation (1996);94:1379-85
Appendix
|
Document Version:
2.0 Lead Author: Dr Sanjay Patel, Infectious Disease Consultant, UHS Additional Authors: Dr Norah Yap, Paediatric cardiology SpR Dr Tara Bharucha, Consultant Paediatric Cardiologist, UHS Dr Alan Magee, Consultant Paediatric Cardiologist, UHS Dr Nick Hayes, Consultant Paediatric Cardiologist, UHS Dr Alice Leahy, Consultant Paediatric Rheumatology, UHS Dr Roy Sievers, Consultant Paediatrician, QAH |
Approving Network:
Wessex Paediatric Infectious Disease Network Wessex Paediatric Rheumatology Network Date of Approval: November 2021 Review Due:
November 2024 |
PIER Contact |
|